 |
Q:
I’ve recently seen some discussion on treating fungal keratitis with rose bengal and photodynamic therapy (PDT). How does this combination’s efficacy compare with riboflavin and corneal crosslinking (CXL)? Are there any indications for one procedure over the other?
A:
“Most optometrists associate PDT with treating wet macular degeneration,” says Brian Chou, OD, of San Diego. He notes that this light-activated treatment’s capabilities don’t stop there. Upon activation, a photosensitizer releases reactive oxygen to targeted cells and tissue to help manage a wide range of conditions, from acne to cancer.
The most recognized form of PDT in eye care is currently CXL for keratoconus and post-LASIK ectasia.1 Riboflavin and ultraviolet (UV) light increase and strengthen molecular bonding between corneal collagen fibrils to prevent progressive ectasia. Other eye-related applications of PDT include corneal neovascularization, microbial keratitis and certain choroidal diseases.2-4
Fungal Keratitis Management
Of the total microbial keratitis cases in the United States, 6% to 20% are fungal.5 The preferred topical treatments are natamycin 5% for Fusarium (filamentous) and amphotericin B 0.15% for Candida (yeast) and Aspergillus (filamentous).6 Due to poor penetrance, deep stromal infections may also require repeated debridement, systemic antimycotics or both, advises Dr. Chou. Even so, he adds that treatment is limited, and resolution often takes months.
PDT is a controversial treatment for fungal keratitis, according to Dr. Chou. Several studies have proposed using rose bengal or riboflavin as the PDT photosensitizer. A team of researchers found that riboflavin and UVA irradiation reduced Fusarium colony-forming units in vitro and improved the clinical appearance of Fusarium keratitis in the in vivo mouse model.7
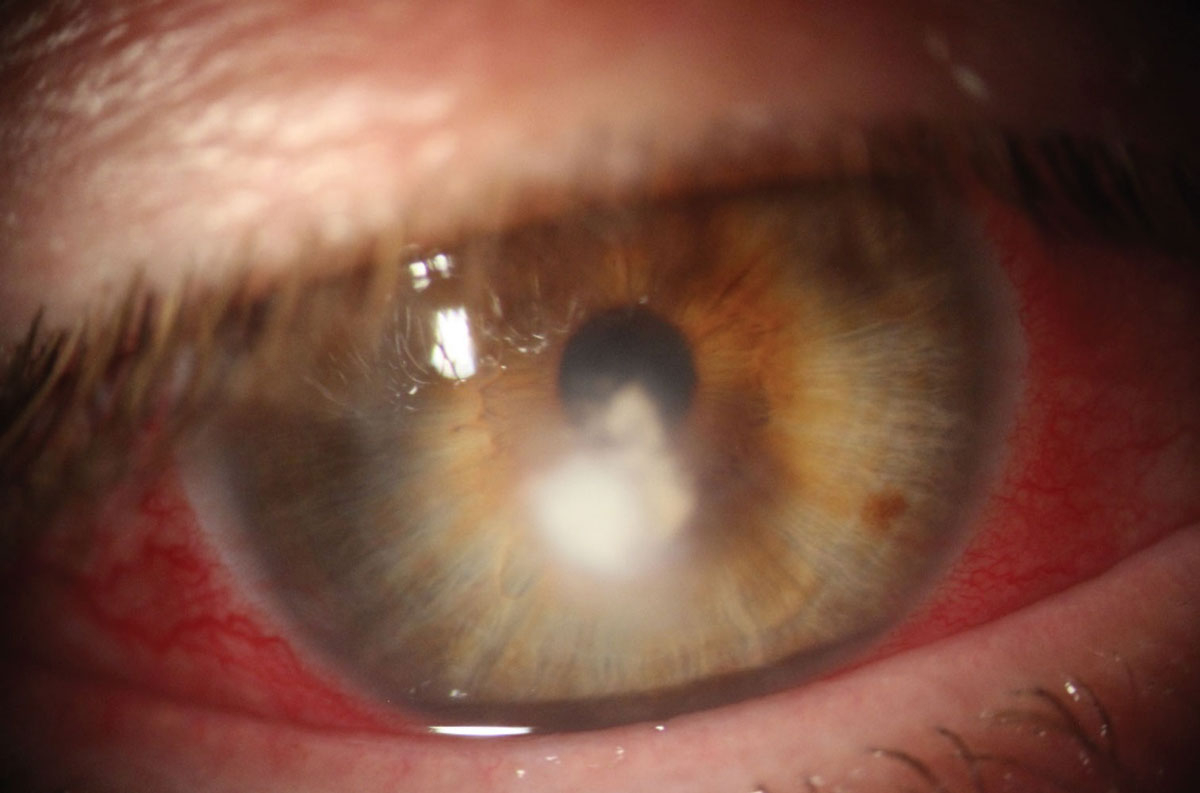 |
PDT with rose bengal can be a suitable option for fungal keratitis treatment. Photo: Delaney Kent, OD, and Richard Mangan, OD. Click to enlarge image. |
However, Dr. Chou says there is greater evidence that the combination of riboflavin and UVA does not effectively inhibit fungal proliferation. A 2017 randomized clinical trial that looked into CXL treatment with riboflavin for deep stromal fungal keratitis was aborted because the clinical group experienced more perforations than the controls.8 Furthermore, recent results of an in vivo clinical trial of 403 patients with filamentous fungal keratitis published in Ophthalmology showed no benefit of adjuvant CXL.9
PDT with rose bengal may offer greater promise, Dr. Chou suggests. In vitro, rose bengal and green light (518nm) effectively inhibited fungal isolates (Fusarium, Aspergillus and Candida), whereas riboflavin with UVA (375nm) permitted unrestricted growth.10 A case report of a 56-year-old rigid gas permeable contact lens wearer with culture-positive Fusarium keratitis described a worsening presentation with hourly natamycin 5%, intrastromal amphotericin B injection and oral fluconazole.11 On day 44, she had rose bengal PDT, and within four days, she had experienced significant improvement.11
Keep rose bengal PDT on your radar, and be on the lookout for more to come on its viability as a treatment option.
1. Lim L, Lim EWL. A review of corneal collagen crosslinking—current trends in practice applications. Open Ophthalmol J. 2018;12:181-213. 2. Yoon KC, You IC, Kang IS, et al. Photodynamic therapy with verteporfin for corneal neovascularization. Am J Ophthalmol. 2007;144(3):390-5. 3. Alio JL, Abbouda A, Valle DD, et al. Corneal crosslinking and infectious keratitis: a systematic review with a meta-analysis of reported cases. J Ophthalmic Inflamm Infect. 2013;3(1):47. 4. van Dijk EHC, van Rijssen TJ, Subhi Y, et al. Photodynamic therapy for chorioretinal diseases: a practical approach. Ophthalmol Ther. 2020;9(2):329-42. 5. Jurkunas U, Behlau I, Colby K. Fungal keratitis: changing pathogens and risk factors. Cornea. 2009;28(6):638-43. 6. Mahmoudi S, Masoomi A, Ahmadikia K, et al. Fungal keratitis: an overview of clinical and laboratory aspects. Mycoses. 2018;61(12):916-30. 7. Zhu Z, Zhang H, Yue J, et al. Antimicrobial efficacy of corneal crosslinking in vitro and in vivo for Fusarium solani: a potential new treatment for fungal keratitis. BMC Ophthalmol. 2018;18(1):65. 8. Prajna VN, Prajna L, Muthiah S. Fungal keratitis: the Aravind experience. Ind J Ophthalmol. 2017;65(10):912-9. 9. Prajna VN, Radhakrishnan N, Lalitha P, et al. Crosslinking-assisted infection reduction: a randomized clinical trial evaluating the effect of adjuvant crosslinking on outcomes in fungal keratitis. Ophthalmology. 2020;127(2):159-66. 10. Arboleda A, Miller D, Cabot F, et al. Assessment of rose bengal vs. riboflavin photodynamic therapy for inhibition of fungal keratitis isolates. Am J Ophthalmol. 2014;158(1):64-70. 11. Amescua G, Arboleda A, Nikpoor N, et al. Rose bengal photodynamic antimicrobial therapy: a novel treatment for resistant Fusarium keratitis. Cornea. 2017;36(9):1141-4. |
