 |
Q:
I have a patient who had radial keratotomy (RK) many years ago who now needs cataract surgery. Are there any special considerations?
“RK, photorefractive keratectomy (PRK) and LASIK can have a profound effect on cataract surgery outcomes,” says Tania Patel, OD, of Commonwealth Eye Surgery in Lexington, KY.
Patients with RK have irregular and fluctuating corneas that can change through the course of the day, affecting initial measurements, IOL calculations and post-op outcomes. The RK cuts that were made change the entire structure of the cornea.1 The integrity of the cornea is never the same with someone who has had RK, no matter when it was performed. LASIK and PRK can also affect cataract outcomes, and patients need to be warned that their post-op journey may not be as smooth.
“I always discuss the whole process with the patient during their initial cataract surgery evaluation,” says Dr. Patel. “I inform the patient that their cornea is irregular from the RK or other refractive surgery and that we modify our formulas and IOL calculations to account for that.” A step beyond formula adjustment is Alcon’s ORA system, which takes intraoperative refraction and wavefront aberrometry measurements prior to lens placement to reduce refractive surprise.
 |
|
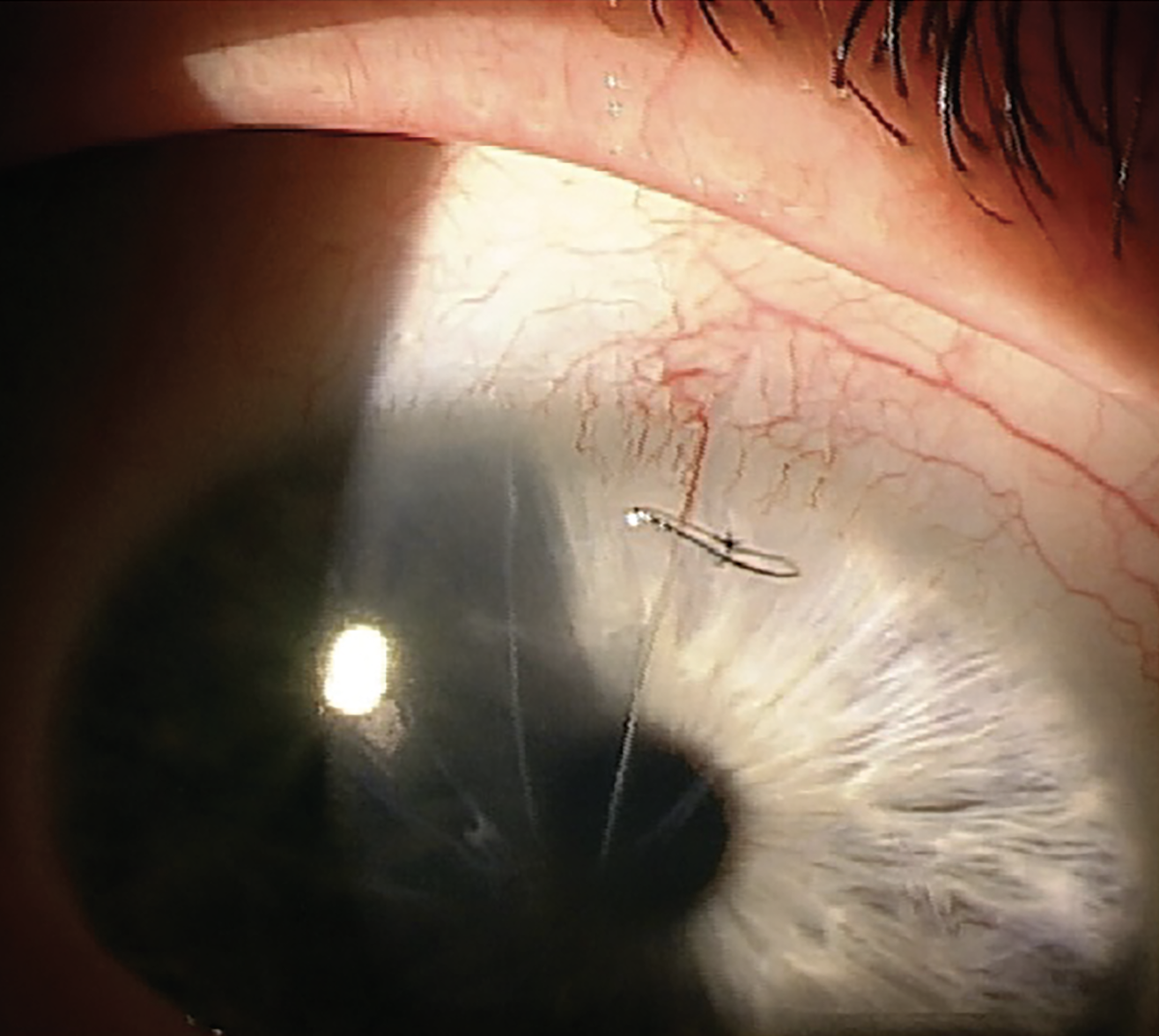
Cataract surgery patient with sutured RK cut. Click image to enlarge. |
Dr. Patel usually does not recommend femtosecond laser-assisted cataract surgery (FLACS) or “premium” lenses in post-RK eyes. Thickened incisional scars are potential sources of incomplete laser penetration, and imperfect ocular surfaces do not fare well with multifocal implants. Toric lens implantation in RK eyes may provide unpredictable astigmatism correction and should be avoided in most cases.2
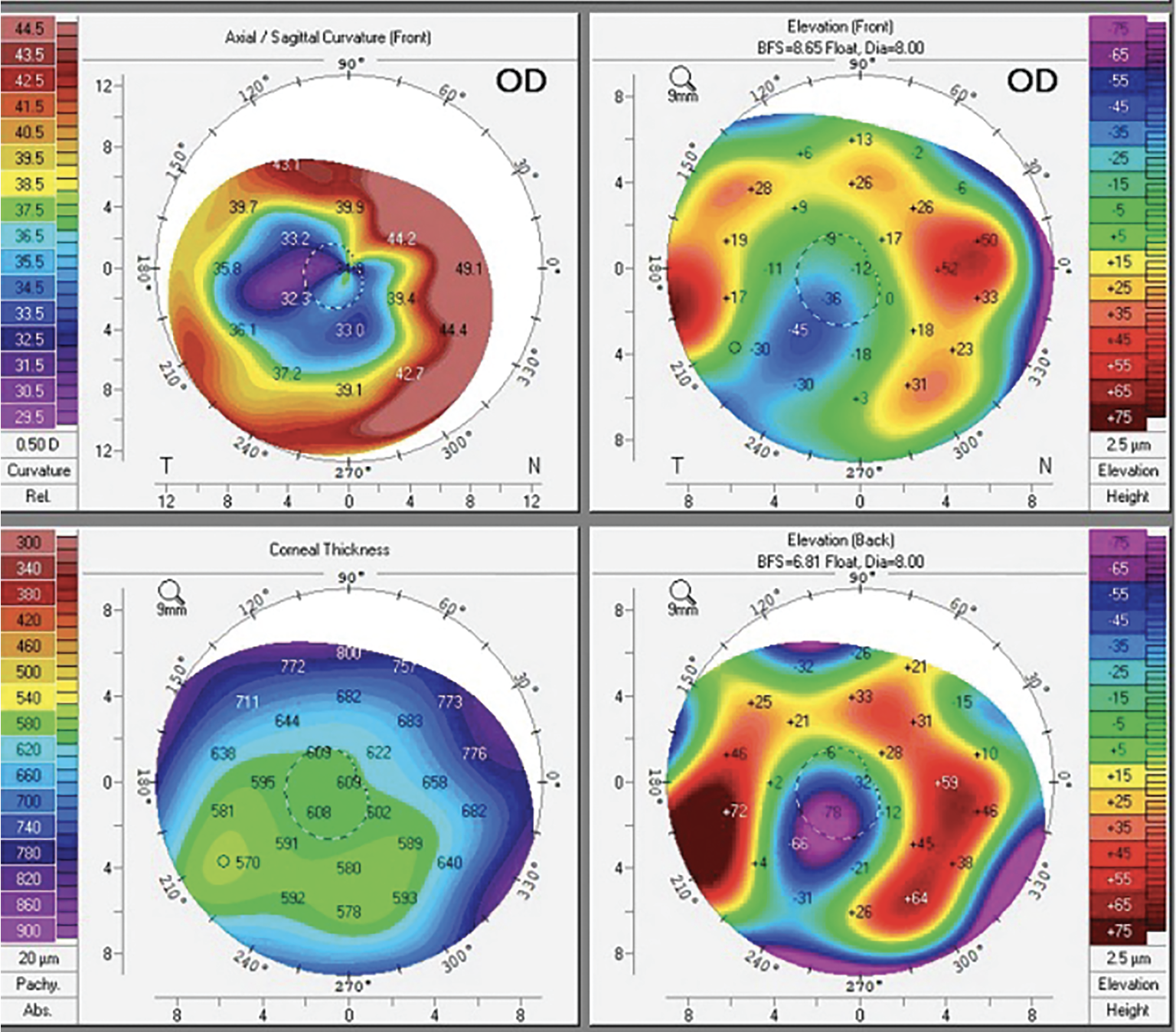 |
| Corneal topography of a patient with RK. Click image to enlarge. |
“The best option for patients with RK is usually a standard monofocal lens,” Dr. Patel says. “We have also had success with the Light Adjustable Lens (LAL) in patients who are status post-RK, -LASIK or -PRK and are willing to pay significant out-of-pocket money for an adjustable monofocal.
Though rare, there is the chance that the RK cuts may open during cataract surgery and require suturing. Higher numbers of RK cuts increase the chance of the cuts unzipping during surgery. With an eight-cut-or-fewer RK incision, the surgeon can usually slip the incisions in between two of the RK cuts. With 12 cuts or more, they may have to revert to a scleral tunnel incision.1
ODs can remove the suture in clinic four to six weeks after surgery using a beaver blade and jeweler’s forceps behind the slit lamp. Prescribe an antibiotic drop or ointment in the eye for a few days following.
“I believe that the most important task for the OD performing the pre-surgical evaluation and then referring the patient for cataract surgery is educating the patient about the possible complications due to their history of RK and LASIK and setting realistic expectations,” Dr. Patel says. “Educate your post-refractive surgery patient that their vision may fluctuate significantly after cataract surgery, and they will need to exercise patience before achieving their final visual goal.” Let the surgeon know what you discussed by sending a detailed referral form or letter, which will make everyone look better in the long run.
Dr. Ajamian is board certified by the American Board of Optometry and serves as Center Director of Omni Eye Services of Atlanta. He is vice president of the Georgia State Board of Optometry and general CE chairman of SECO International. He has no financial interests to disclose.
1. Stephenson, M. Cataract/IOL surgery after RK. Rev Ophthalmol. 2021;28(10):38-40. 2. Trinh T, Solomon B, Mimouni M, et al. Outcomes of femtosecond laser-assisted cataract and refractive lens surgery in patients with prior radial keratotomy. J Cataract Refract Surg. 2022;48(4):449-55. |
