 |
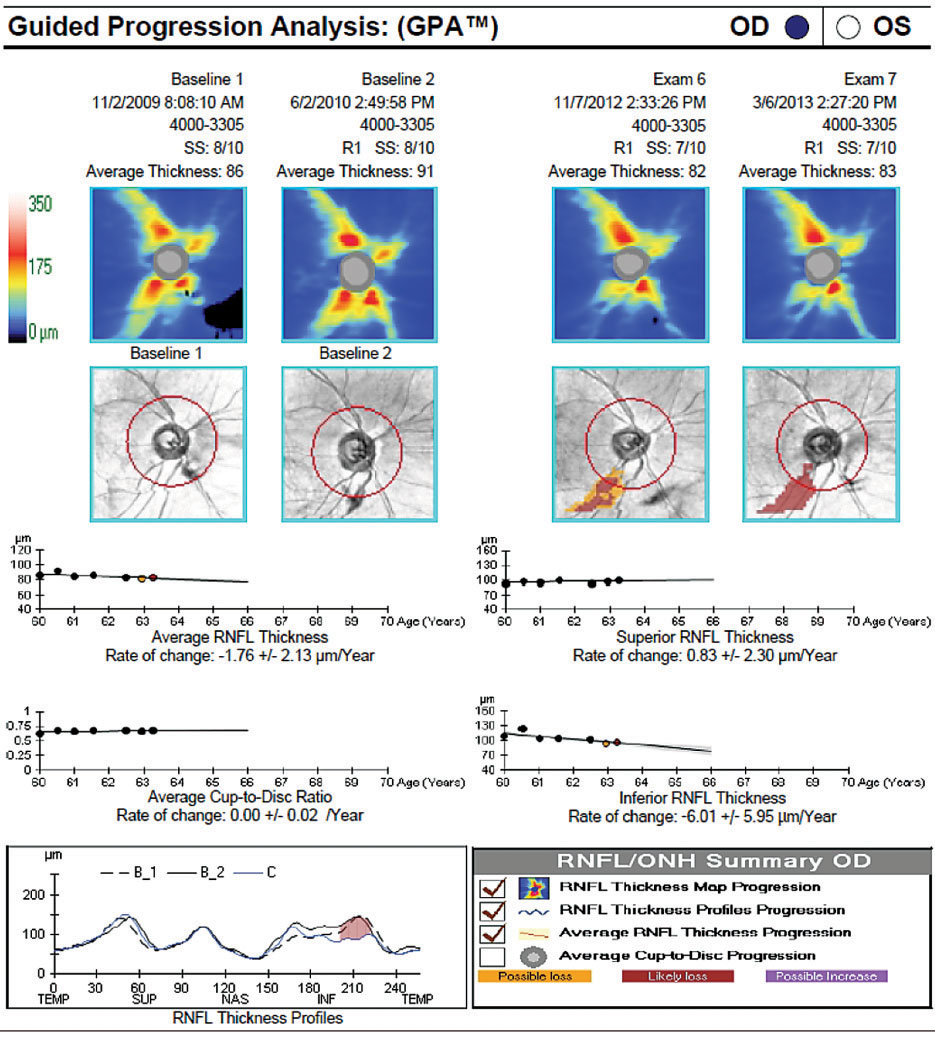
| Faster rates of RNFL thinning were also present in advanced glaucoma but statistical significance was limited by the lower sample size of eyes above target and the OCT floor effect. Photo: Danica J. Marrelli, OD. Click image to enlarge. |
There is a limited understanding of the real-world impact of achieving the clinician-set target pressure on glaucoma progression. Much of the work was conducted as clinical trials with pre-defined protocols that may not represent actual practices and patients in a real clinical population. Additionally, pre-specified levels of IOP control do not consider the clinician's knowledge and experience when setting target pressures. A recent study based out of the Wilmer Eye Institute at Johns Hopkins University in Baltimore, MD, sought out to determine whether target difference has a greater impact on rates of glaucoma worsening observed through OCT scans than absolute levels of IOP, as well as investigate the impact of disease severity on these relationships. When eyes were above their clinician-set target pressure, they had significantly faster rates of RNFL worsening. Each 1mm Hg increase above the target pressure had a greater impact on RNFL worsening than each 1mm Hg increase below the target pressure and each 1mm Hg increase in mean IOP.
The retrospective cohort study, published in American Journal of Ophthalmology, included 3,256 eyes (1,923 patients) with ≥ five reliable OCT scans and one baseline visual field test. Eyes below and above target had significantly different mean RNFL slopes (-0.44µm/year vs. -0.71µm/year). Each 1mm Hg increase above target had a 0.143µm/year faster rate of RNFL thinning. Separating by disease severity, suspect, mild, moderate and advanced glaucoma had 0.135µm, 0.116µm, 0.203µm and 0.65 µm/year faster rates of RNFL thinning per 1mm Hg increase, respectively.
When comparing the relative percentage decrease from the baseline, the percentage reductions support the conclusion that clinically treated eyes that achieve their target pressure experience slower or similar rates of RNFL loss to healthy eyes and that eyes above target pressure experience faster rates that could potentially result in a higher risk of future VF progression. Eyes below the target pressure experienced a 0.30% per year decrease in RNFL thickness. The corresponding normal age-related changes cited above equate to a 0.16% to 0.52% per year RNFL decrease. In contrast, eyes above target pressure experienced rates of RNFL thinning that was more than twice as fast with a 0.70% per year decrease.
“Eyes with early glaucoma and minimal VF loss may have notable RNFL thinning that can be readily detected,” the authors wrote in their paper. “However, as the RNFL continues to thin and begins approaching the measurement floor of OCT imaging, such as in eyes with advanced glaucoma, it becomes more difficult to detect changes in the RNFL thickness.”
“As an observational study, our data were obtained from clinical records, so our findings reflect associative relationships and not causal ones,” the research team emphasized. “The models chosen for this study assume a linear relationship between the primary independent variables and dependent variables because of their traditional use in glaucoma literature.”
Pham AT, Bradley C, Hou K, et al. The impact of achieving target intraocular pressure on glaucomatous retinal nerve fiber layer thinning in a treated clinical population. Am J Ophthalmol. November 27, 2023. [Epub ahead of print]. |
