 |
|
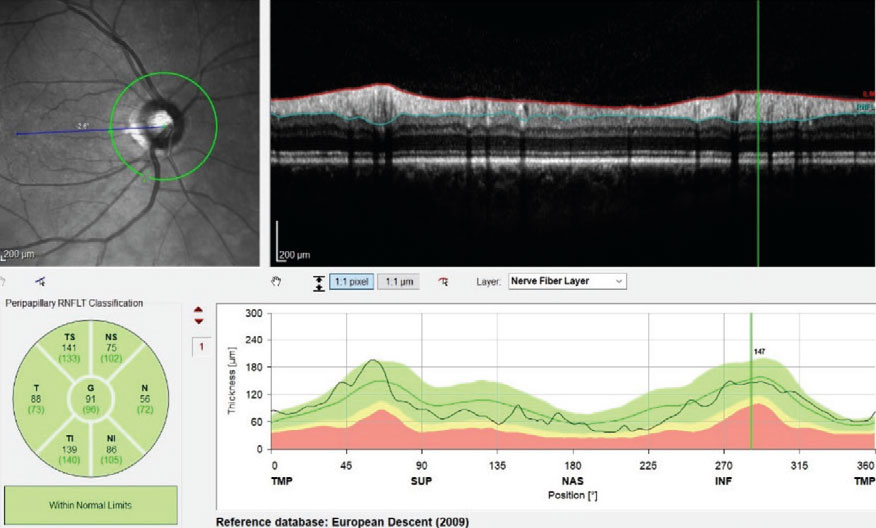
Beware of false-positive (“red disease”) and false-negative (“green disease,” shown above) results when grading OCT scans using manufacturer-provided normative datasets, as some were developed without taking influential factors such as age, sex and refraction into account. Photo: James Fanelli, OD. Click image to enlarge. |
Normative datasets provided by OCT manufacturers are intended to improve the detection and monitoring of various ocular diseases, including glaucoma, by color-coding data as normal (green), borderline (yellow) and abnormal (red); however, in some cases, these plots produce false-positive (“red disease”) or false-negative (“green disease”) results, leading to misinterpretation of clinical data. These resources have also been criticized as unrepresentative of ethnic, gender and age diversity of the population. Such shortcomings have led many clinicians to favor the more neutral term reference database over the still-common label normative database.
Researchers recently found that when predicting glaucomatous field loss with retinal nerve fiber layer thickness (RNFLT) measurement, so-called normative percentiles don’t provide any additional value over raw RNFLT data.
The longitudinal study included OCT scans and visual fields from patients of the glaucoma clinic at Massachusetts Eye & Ear. Spectralis OCT normative distributions were obtained from machine printouts and found to be independent of patient-specific parameters such as age, sex and ocular magnification. Machine learning models were then used to compare the predictive performance of percentile RNFLT and raw RNFLT inputs.
The analysis of 3,016 OCT-visual field pairs that met the reliability criteria showed a significant decrease in R2 from predictive RNFLT models compared to raw RNFLT models in inferotemporal sectors, across multiple regressors. Additionally, no significant improvements in ROC-AUC scores were noted between the two types of data.
The researchers made an interesting observation in their paper on the study that may hint at the reason why normative datasets didn’t have as much predictive ability as raw data. “Inspection of regional regression plots suggest that raw RNFLT inputs preserve a trend with mean deviation across the thickness range, whereas percentile inputs only show a consistent relationship below the 20th percentile,” they wrote. “The percentiles might lose information that is still contained in the original thickness data. Above the 20th percentile, the relationship is flat, including a broad range of patients with moderate to severe visual field loss. The Spectralis percentiles may maintain high specificity but show decreased sensitivity for moderate to severe glaucoma.”
The absence of age, sex and ocular magnification from the reference database on the Spectralis OCT could also contribute to the lack of noted improvement over raw data, the study authors suggested. “Normative data should include factors that influence RNFLT, such as age, sex and refraction,” they wrote in their paper, adding that they encourage OCT manufacturers to “provide detailed information about demographics of reference populations for normative databases.” Including this information could help establish more robust norms and reduce clinical instances of “red disease” and “green disease”, they suggested.
Until there is greater validation of norms on OCT devices, the researchers advise clinicians to interpret these reference datasets with caution.
Singh R, Rauscher FG, Li Y, Eslami M, et al. Normative percentiles of retinal nerve fiber layer thickness and glaucomatous visual field loss. Tran Vis Sci Technol. 2023;12(10):13. |
