 |
In previous columns, we have discussed in detail the use of plus lenses to help abate the signs and symptoms of near point stress. Regardless of the examination findings, when considering the prescription of plus at near, whether in the form of a near vision, bifocal or progressive addition lens, it is important to document some aspect of improvement. This positive change can be objective, subjective or both. This month, we will differentiate the two and discuss the go-to tests we use to demonstrate changes that help guide our decision-making when it comes to plus at near.
Of course, in a perfect world, we trial frame the proposed plus at near and the previously poor data improves to normal values and the patient jumps up and down, claiming we are miracle workers. In reality, the improvement is not always as robust and can actually be quite subtle.
Objectively, we typically hear things like, “the print got larger,” “my eyes do not feel as strained” or “my eyes feel more relaxed.” The key is that the change is in the positive direction. We rely on the patient using their words, not ours, to describe this change. For example, they may not say that something became larger or smaller but that their eyes are working harder or easier. Try your best to not “lead the witness” as they say on TV. There are times in which you need to probe with some tests. Some patients, especially younger ones, do not know how to describe the change that has taken place. When probing, steer clear of only asking questions that yield positive answers; present both sides equally and perhaps even concentrate on the middle of the spectrum of possibilities.
Keep in mind that the longer the adaptation to the near point stress takes, the less likely you are to receive an immediate positive verbal response. These cases may not yield big or early changes in the vision therapy room, and the patient may need more time to recognize the impact of the lenses.
Subjectively, there are so many tests to choose from to determine the impact of plus lenses. The key is to focus on one or two on which the patient performed poorly. Certain test results indicate that plus at near would be beneficial, so we suggest using these to confirm evidence of improvement:
Stereo Testing
There are many variations of stereo tests. Whether you like the Random Dot Stereo Test with a mixture of local and global targets or the Random Dot 3 Stereo Test with all global targets, a reduction is considered an indication of a visual efficiency issue. Retesting with trial lenses is a simple and effective way to determine an immediate impact. For example, if the stereo improves from 70 to 30 sec, you have your objective data.
Near Point of Convergence
While a reduced NPC is often associated with a convergence insufficiency, it is not pathognomonic for it. A reduced NPC is indicative of a binocular or accommodative disorder, so disregard the unwritten rule that a patient with a convergence issue cannot benefit from plus at near. If there is an accommodative issue compounding the convergence dysfunction, it is very likely that plus will be of benefit. We have also found that if the NPC reduction increases with repetition, plus is more likely to help. Repeat the NPC with the potential plus lenses for proof of improvement.
Cover Test/Phoria at Near
The expected near posture as determined by either the cover test or von Graefe phoria is 4.00 to 6.00 prism diopters of exophoria. An indication of the need for plus at near would be esophoria or even orthophoria, which should be considered a relative esophoria. If plus lenses are impactful, upon retesting there will be movement toward the ideal 6.00 prism diopters of exophoria. While in a perfect world, the plus will get the patient into the desired exo range, nudging them in the right direction can go a long way and set the stage for success in the vision therapy room.
NRA/PRA
Negative relative accommodation (NRA) and positive relative accommodation (PRA) assess both accommodation and binocularity. An imbalance in which there is a higher NRA (+) than PRA (-) shows the potential for improvement with plus. This pair of tests is also helpful in providing a starting point for our plus journey. For example, if the NRA/PRA is +2.50/-1.00, the difference is +1.50. Half of that difference, or +0.75, should be your starting near plus prescription. Retesting the NRA/PRA should show better balance if you use this add power, which can then be assessed with any of the tests we cover here and a multitude of others.
Near Point Retinoscopy
While we don’t specify the type of near point retinoscopy, as everyone has their personal preference, the concept of using any of these methods to determine plus acceptance is similar. If the near retinoscopy shows a lag of accommodation of higher plus than +0.25 to +0.75, plus should be considered. As we always strive to leave the patient with the normal near retinoscopy of +0.50, anything in excess could be trialed at near.
|
|
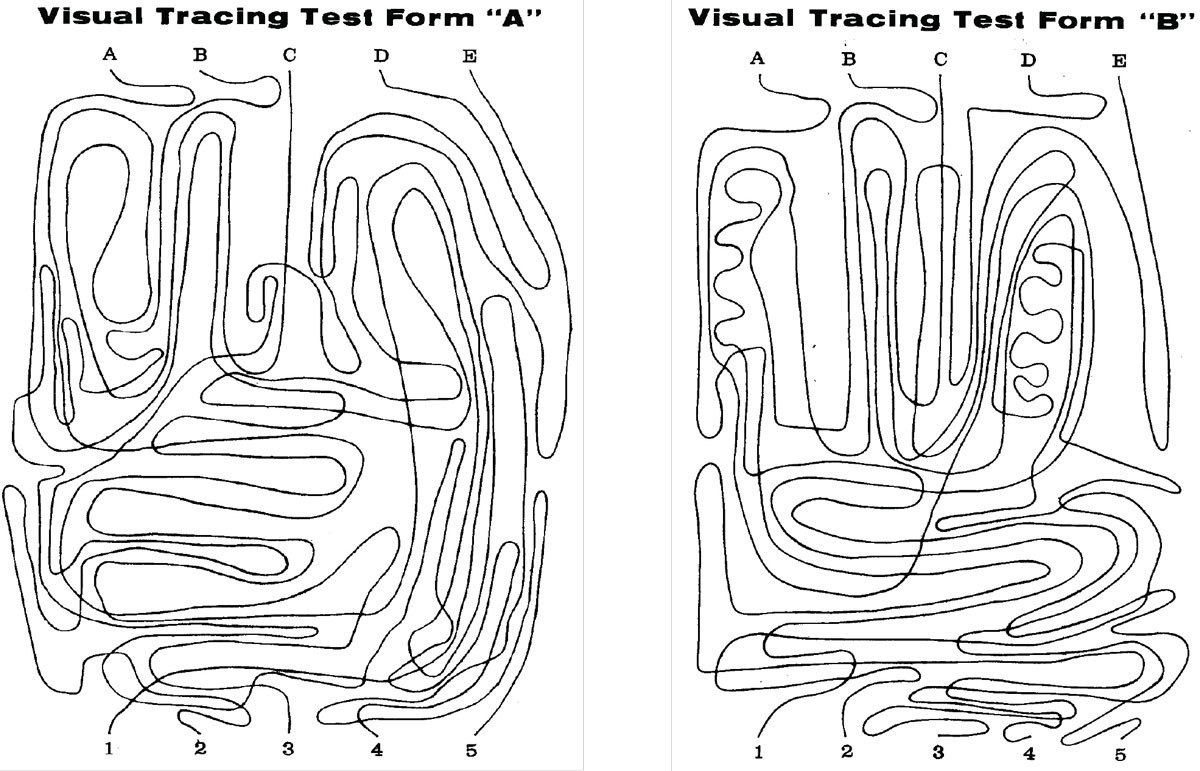
The Groffman Tests A (left) and B (right) are examples of visual tracing exercises that can help determine the impact of plus lenses. Click image to enlarge. |
Groffman Visual Tracing Test
You might assume that this is a test of tracking, but in actuality it is so much more. It consists of five intertwined lines beginning at letters at the top of the page and ending on numbers at the bottom. We time the patient while they track each of the five lines from the top to the bottom. If a child performs well below what is expected at their age as part of routine performance testing, we will often grab a pair of plus lenses and have them repeat the test with a second set of lines. If there is an improvement in time or the number of correct trackings, this is a good sign the lenses will be beneficial. We have seen patients perform three- to five-times better on this test with the plus.
ReadAlyzer Test
Children are commonly referred for poor reading performance. Aside from shorter, number-based tests, the ReadAlyzer (Bernell) is the gold standard. With built-in sensors, we can finally understand the eye movements that take place while reading. Nearly 10 years ago we conducted a study at the Southern College of Optometry that showed an increase in reading speed with improved reading comprehension with the addition of a plus lens.1 The reading speed increased by 3%, but it resulted in a 6% improvement in comprehension.1
Takeaways
While we presented these tests separately, one does not make or break the use of plus lenses at near. Using a combination of evaluation methods and all of the data points collected will lead the clinician closer to a subjective and/or objective patient response. If the improvement is nonexistent or minimal, vision therapy is always an option.
Dr. Taub is a professor, chief of the Vision Therapy and Rehabilitation service and co-supervisor of the Vision Therapy and Pediatrics residency at Southern College of Optometry (SCO) in Memphis. He specializes in vision therapy, pediatrics and brain injury. Dr. Harris is also a professor at SCO. Previously, he was in private practice in Baltimore for 30 years. His interests are in behavioral vision care, vision therapy, pediatrics, brain injury and electrodiagnostics. They have no financial interests to disclose.
1. Iyer, J, Harris, P. The effect of low plus lenses on reading rate and comprehension. Optom Vis Perf. 2013;1(2):59-61.
