While uveitis comprises a diverse group of inflammatory eye diseases, those involving the macula account for a disproportionate amount of visual impairment and blindness. Consequently, is it vital to continue researching potential effective therapies for noninfectious uveitis, despite the low US prevalence of around 115 affected per 100,00 people. A new assessment conducted at the behest of the American Academy of Ophthalmology as one of its periodic Ophthalmic Technology Assessments, explored the role of anti-inflammatories.
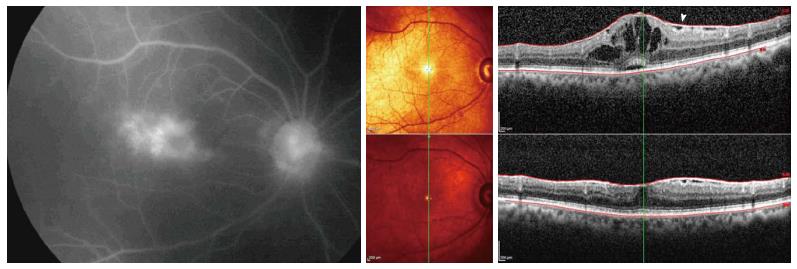 |
| The leading cause of moderate or severe vision loss in uveitis are macular edema and macular scarring often secondary to macular edema. Photo: Shoughy SS, et al. World J Ophthalmol. 2014; 4(3):56-62. Click image to enlarge. |
One of the most basic principles in managing noninfectious uveitic macular edema is to gain control of intraocular inflammation; systemic anti-inflammatory options are often initiated as treatment then transitioned. However, different preparations of corticosteroids for intraocular delivery have recently been introduced, including triamcinolone acetonide for intravitreal injection, intraocular dexamethasone and fluocinolone acetonide implants and suprachoroidal triamcinolone acetonide depot.
With the emergence of these new methods, a team of experts wanted to investigate the effectivity and complication rates of periocular and intraocular corticosteroid therapies. Conducting a meta-analysis, the researchers included a total of 23 articles (providing level I or II evidence) from 18 studies on periocular, suprachoroidal and intravitreal triamcinolone acetonide injection use as well as fluocinolone acetonide implants or inserts for noninfectious uveitis macular edema.
Consistently demonstrated across reports was that all periocular and intraocular corticosteroid therapies improved visual acuity, macular structure or both. In one comparative study, intravitreal triamcinolone acetonide injections and dexamethasone intravitreal implants yielded greater effectivity than periocular triamcinolone acetonide injection. However, when the studies were taken together, an apparent potential for these therapies was highlighted to elevate intraocular pressure and accelerate cataract formation.
Overall, clinical relevance of these results can be summarized as providing “high-quality evidence that periocular and intraocular corticosteroid therapies are effective and safe for the treatment of noninfectious uveitic macular edema. However, information on the relative effectiveness and complication rates across the different therapies is limited.”
Upon further discussion, the authors add that information on fluocinolone acetonide therapy effectivity is limited for the most recently marketed and relatively lower-dosed intravitreal insert due to articles focusing on noninfectious uveitis in general. Also noted is that patients are often treated simultaneously with other therapeutics in these uveitis therapeutic clinical trials, potentially impacting clinical outcome. Reports mainly focused on reporting adverse events of intraocular pressure changes and cataract, but these also reflect the most common drug-related complications across these therapies.
Further research is needed on these periocular and intraocular corticosteroid therapies, which the authors suggest should focus on expanding comparisons of effectiveness and complications among the different options. Particularly, this should include suprachoroidal triamcinolone acetonide injections and intravitreal fluocinolone acetonide implants and inserts since both have only been assessed in isolation.
The researchers add that, “given the potential for certain biologic immunomodulatory drugs to resolve uveitic macular edema, combinations with locally delivered corticosteroid therapies represent a potentially impactful area of research.”
Smith JR, Thorne JE, Flaxel CJ, et al. Treatment of noninfectious uveitic macular edema with periocular and intraocular corticosteroid therapies. Ophthalmology. April 21, 2024. [Epub ahead of print]. |
