 |
Visual acuity and contrast sensitivity deteriorated in every group, proving that rehabilitation of an inherently progressive condition such as AMD is challenging. Photo: Yow AP, et al. 2018 IEEE Engineering in Medicine and Biology Society. Click image to enlarge. |
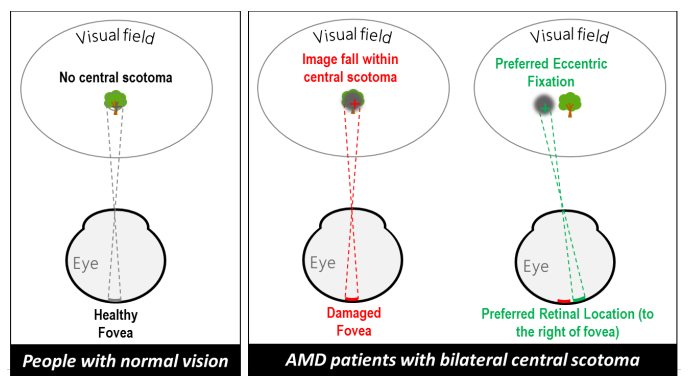
People with macular disease that manifests central vision loss must train themselves to use non-central retina viewing targets to compensate. If one retinal area is used in place of the damaged fovea, it is known as the preferred retinal locus. Fixation is less stable when using non-central retina. This sometimes involves those affected developing a new, trained retinal locus, usually in the superior retina, above the scotoma or the part of the retina with best visual acuity. Training can change the preferred retinal locus location, although this may have a negative effect on reading performance. Eccentric viewing training for macular disease has been performed for more than 40 years, but no large studies including control groups have assessed the benefits of this training.
A group from the NIHR Biomedical Research Center of Moorfields Eye Hospital in London presented the results of the Eccentric Fixation From Enhanced Clinical Training (EFFECT) study, a large randomized controlled trial comparing two models of eccentric viewing training: training at the preferred retinal locus and biofeedback training at a trained retinal locus. They found no effect of eccentric viewing training on task ability, reading performance or fixation stability. On average, visual acuity and contrast sensitivity deteriorated in every group, reflecting the difficulty of rehabilitation in a group of people with an inherently progressive disease and suggesting that disease progression outweighed any benefit of training.
The trial randomized 200 adults with AMD to either: (1) a control group; (2) a group receiving supervised reading support; (3) a group receiving three sessions of training to optimise the use of their own preferred retinal locus; or (4) a group receiving three sessions of biofeedback training of a theoretically optimal trained retinal locus. All participants received standard low vision rehabilitation.
The researchers noted that the patients received three 45-minute training sessions in this study. “There is wide variability in the amount of training suggested by other authors, ranging from eight 10-minute sessions to 30 to 60 hours over up to six weeks,” they wrote in their paper, which was published in Ophthalmology Science. “More training may have led to more impressive outcomes in this study, but the lack of any effect after 135 minutes of training does not suggest this.”
In the study, eccentric viewing training was performed by experienced low vision optometrists, who received additional instruction from a very experienced eccentric viewing trainer. However, they did not have direct clinical experience of the technique before this study. “More experience of eccentric viewing training may lead to better outcomes,” the researchers proposed.
“In our large, carefully controlled, randomized clinical trial we found no effect of eccentric viewing training on task ability, reading performance or fixation stability,” the paper concluded. “Our results do not support the routine provision of eccentric viewing training for people with progressing AMD.”
Rubin GS, Crossland MD, Dunbar HMP, et al. Eccentric viewing training for age-related macular disease: Results of a randomized controlled trial (the EFFECT study). Ophthalmol Sci. October 30, 2023. [Epub ahead of print]. |
