Practical Matters in Myopia Management - 3rd EditionWith an expanding arsenal of information, myopia can be a puzzling area of care. In this third annual Review of Optometry supplement, experts offer solutions backed by science to help you manage this growing patient population. Click here to download a PDF or here to read the digital edition. Check out the other articles featured in this supplement: |
While randomized clinical trials are at the top of the evidence-based pyramid and provide important information for managing many myopic children, numerous patients fall outside of this range and even the “textbook cases” require a highly patient-specific approach. This article will discuss approaches to more challenging clinical cases and how to understand different levels of research evidence to help you practice at the forefront of myopia management.
Case 1: Pre-myopia
A seven-year-old Caucasian girl presented for a myopia management consultation. Her manifest refraction was the same in each eye: +0.50 -0.50x180. She is adopted, so her family history is unavailable—but she is an avid reader.
With myopia becoming more of a public health concern, it is not wholly uncommon for parents to ask about myopia management therapies before their child is even diagnosed. Pre-myopia is defined as ≤ +0.75D and > -0.50D with other identifiable risk factors that will likely lead to future myopia development.1 This is a critical period when the child has not fully developed myopia, so interventions are imperative to help delay its onset. Refractive error is one of the most important risk factors to look at during this time. Having a hyperopic buffer can lower the risk of developing myopia, such that a child should be ≥ +0.75D at age six, ≥ +0.50D at age seven to eight, ≥ +0.25D at age nine to 10 and emmetropic at age 11.2 If a child is more myopic (i.e., less hyperopic) at any of these stages, they are likely to develop myopia.
During this delicate time, it is vital to remember that myopia prevention is the primary goal. By delaying myopia onset for one year, the myopic level of the patient can be reduced by 0.75D or more.3 This one-year delay can also equate to the effect achieved by three years of active myopia control. From a financial and lifestyle standpoint, this impact can be significant. Therefore, practitioners need to identify and educate parents and patients before the onset of myopia.
Both genetic and environmental factors contribute to the development of myopia. With one myopic parent, the risk of a child developing the condition is three times greater than with no myopic parents; this risk increases to six times greater if both parents are myopic.4 While genetic factors cannot be changed, behavioral factors affecting the visual environment can. Increasing time outdoors to two hours per day or 10 hours per week can delay the onset of myopia.5 Additionally, decreasing the intensity of near work, rather than the total duration, can also postpone onset. Near-work intensity can be reduced by increasing working distances to greater than 30cm and increasing the number of breaks so that time spent on continuous reading is no more than 30 minutes.6Axial length is the gold standard for monitoring myopia progression, but it is not routinely performed on our non-myopic patients. The COMET study showed that an increase in axial elongation occurs two to three years prior to the onset of myopia.7 Therefore, it may be helpful to monitor axial elongation in pre-myopic patients.
Thorough parent and patient education on myopia risk factors, development and myopia control therapies should be implemented before myopia onset. Behavioral modifications such as increasing outdoor time and decreasing near work intensity should help delay myopia onset. Shorter follow-up periods may be recommended so myopia control therapies can be initiated as soon as the myopia diagnosis is made. More recently, the use of atropine to treat pre-myopia has been explored. Three studies done in Asia have all found that using atropine of varying concentrations resulted in a lower incidence of myopia compared with placebo or no treatment.8-10 The use of special defocus-inducing myopia control spectacles is also being explored for pre-myopia.11
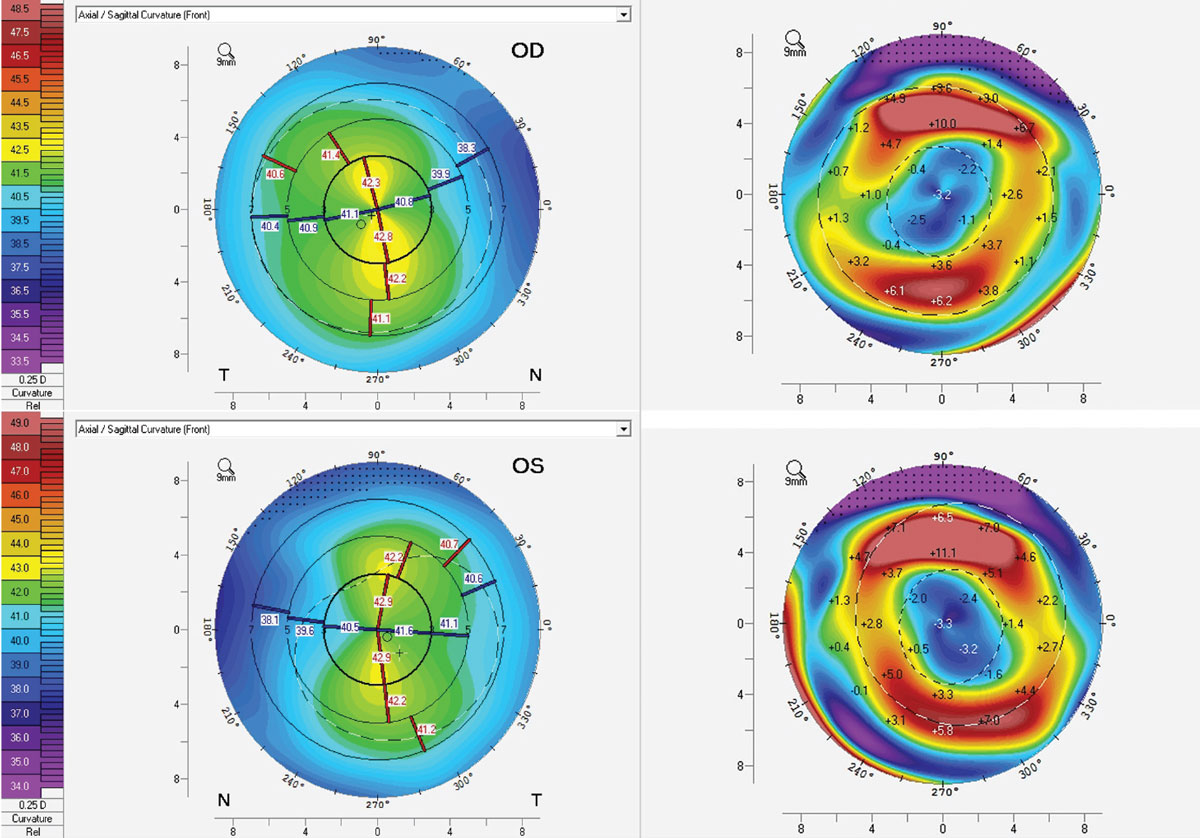
Conclusion. Recommendations for increased outdoor time, increased near-working distance and decreased time spent on continuous near work were made at the initial consultation, with a shorter follow-up time to monitor for potential myopia progression. After 1.5 years, the patient returned with a slight increase in myopia, and orthokeratology (ortho-K) treatment was initiated (Figure 1).
 |
|
Fig. 1. Corneal topography showing mild apical with-the-rule astigmatism (top and bottom left) and adequate treatment with ortho-K (top and bottom right) both OD (top left and right) and OS (bottom left and right). Click image to enlarge. |
Case 2: High Myopia in a Teen
The manifest refraction for a 15-year-old Asian girl was -6.25D OD and -5.50 -0.50x170 OS. Her keratometry readings were 46.35D @ 016 / 47.66D @ 106 OD and 46.79D @ 162 / 49.17D @ 072 OS. Her parents were interested in initiating myopia control with ortho-K lenses.
Parents often ask how long their child will need to use myopia management therapies. The COMET study evaluated over 400 myopic children of varying ethnicities over 11 years and found that the average age of stabilization was 15.6 years with a mean refractive error of -4.87D.12 However, there was a large variation in the age of stabilization. About half of children reached stabilization at age 15, while 75% reached it by age 18, 90% by age 21 and 95% by age 24. Conversely, this means 50% of children continue to progress past age 15 and 5% by age 24.
Customizing ortho-K lens parameters can help maximize treatment efficacy for high myopes. Initial studies have shown that a smaller optic zone size (5mm vs. 6mm) slows axial elongation. This is perhaps due to the fact that there is more peripheral plus power or spherical aberrations induced within the pupil margins, providing more consistent treatment effect.13
Besides changing the optic zone diameter, increasing the compression factor can accelerate corneal reshaping and allow the patient to achieve better visual acuity faster.14 The increased compression factor will result in less residual myopia by one week and better initial high-contrast visual acuity at the one day follow-up. These initial results are helpful for high myopes to feel confident and successful with ortho-K lens wear, but the benefits of an increased compression factor are only temporary as the refraction and unaided visual acuity are no different than with a lower compression factor over time. The increased compression factor also has no influence on myopia control.15
Fitting ortho-K lenses may be a little more challenging with high myopes. For such patients with already high axial length measurements, parents may wonder if it is still possible to slow eye growth. Studies have shown even with high myopia, wearing ortho-K lenses indeed is still able to achieve slowing of axial length growth.16,17 There is also potential value in using ortho-k for partial correction in high myopes or combining with atropine to enhance axial length control.18,19
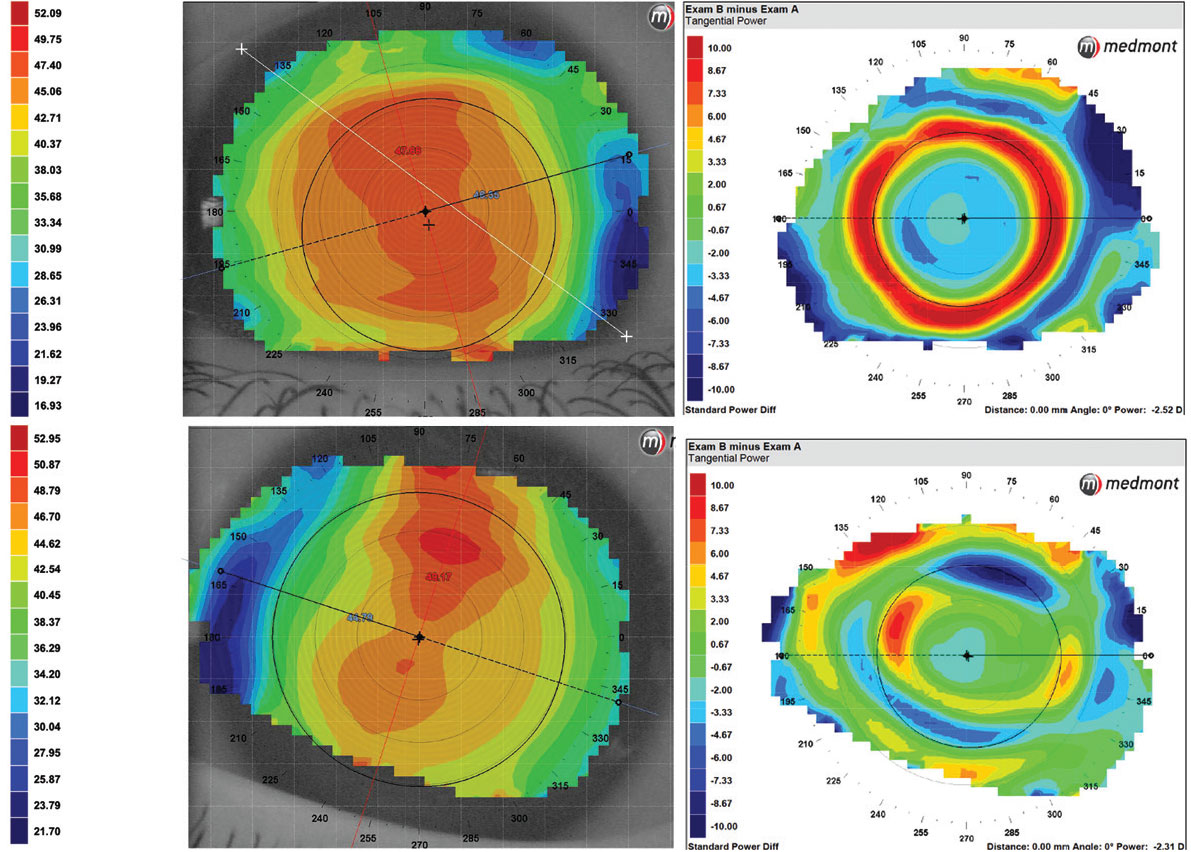
Conclusion. Though the patient was already 15, her myopia could still potentially progress, so it was important to initiate ortho-K lens wear (Figure 2). Her refractive error was already at the upper limit of correctable myopia, but she had steep corneas to allow for central flattening. In fact, her steep corneal curvatures may be suspicious for early keratoconus, so it would be worthwhile to perform corneal tomography to evaluate the posterior float.
 |
|
Fig. 2. Corneal topography at baseline visit (top and bottom left) and after ortho-K (top and bottom right) both OD (top left and right) and OS (bottom left and right). Click image to enlarge. |
Case 3: High Astigmatism
Parents brought in their nine-year-old Asian son for a comprehensive examination. He was prescribed his first pair of glasses at age five. His father is a moderate myope, and his mother is emmetropic. His manifest refraction was -5.25 -2.25x180 OD and -4.75 -2.25x180 OD. His keratometry readings were 43.4D @ 010 / 45.8D @ 100 OD and 43.5D @ 175 / 46.5D @ 085 OS.
Early studies evaluating spherical ortho-K on astigmatic patients showed the treatment could correct up to half of the pre-treatment toricity.20 This study only included 23 eyes, though, and showed residual astigmatism is expected with spherical ortho-K.
There are ortho-K lenses available now with toric periphery designs. In these, the base curve is spherical but the peripheral curves are toric to improve centration and alignment. This improved lens centration makes ortho-K treatment more effective for patients with high astigmatism.
Limited research has been done on astigmatic myopia control therapies. A direct comparison of soft toric multifocal lenses and toric ortho-K lenses showed greater induced higher-order aberrations and more peripheral myopic defocus with toric ortho-K lenses.21,22 Participants found comparable comfort between both modalities but there was a preference toward vision with ortho-K lenses.23
Fitting patients with high astigmatism can be more challenging. Proper fitting, patient education and lens evaluation are critical in managing these patients. It is crucial that the practitioner, parent and patient have realistic expectations for the fitting process and visual outcomes, understanding that it may require additional chair time and there will be residual astigmatism. Providers may also consider combining different treatments to maximize vision correction, including soft multifocals for myopia control with single vision spectacles to correct for astigmatism.
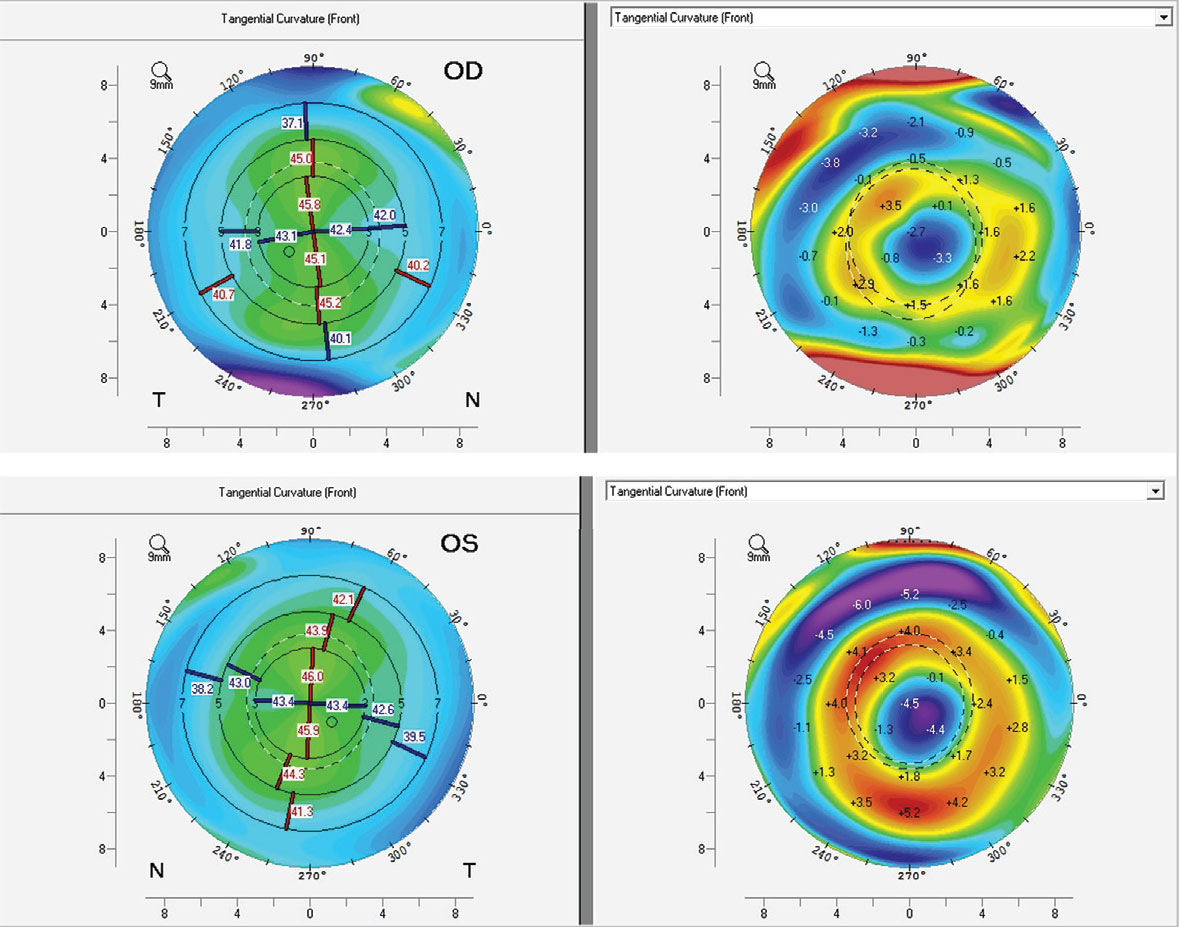
Conclusion. This patient was fit with toric ortho-K lenses (Figure 3). He achieved 20/20 visual acuity OU and has been successful with lens wear for over one year with no axial elongation or change to his contact lens parameters. One consideration for discussion is that this patient is already approaching the maximum limit of myopic correction at a relatively young age, so he may not be able to sustain treatment with ortho-K and, in the future, may need to switch modalities or continue with partial treatment, which would require he resume spectacle lens wear.
 |
|
Fig. 3. Baseline corneal topography (top and bottom left) and after ortho-K wear (top and bottom right) both OD (top left and right) and OS (bottom left and right). Click image to enlarge. |
Case 4: Combining Treatments
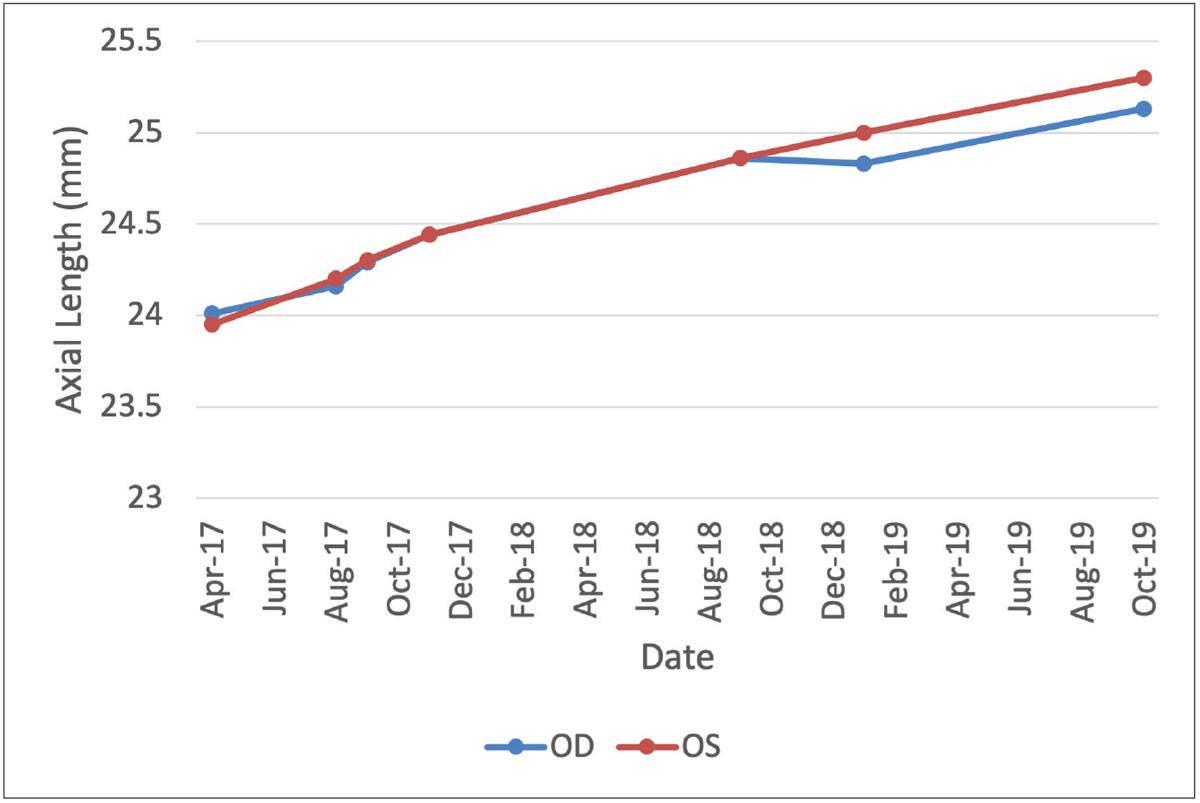
When this patient first presented, he was a seven-year-old Asian boy with a manifest refraction of -2.00 -0.75x037 OD and -2.00 -0.75x003 OS. After discussing all potential treatments, his parents selected soft multifocal lenses. After a year of noncompliance, the patient switched to ortho-K lenses. The patient was still inconsistent with lens wear and axial length progression was noted (Figure 4).
Few studies have been conducted regarding switching or combining different myopia control therapies. Adding atropine 0.01% to ortho-K slows axial elongation more than either therapy alone.24,25 Particularly, dual therapy may help the patient achieve a boost in efficacy during the first six months. However, adding atropine to ortho-K in poor responders does not enhance outcomes.26 Therefore, combining ortho-K and low-dose atropine may be more effective than monotherapy, but the amount of axial length slowing is not double and is greatest during the initial period.
Only one study has examined combining atropine 0.01% with soft multifocal lenses and found that it is not more efficacious than using soft multifocal lenses alone.27 More research is needed to support these findings, particularly with different multifocal lens designs.
Lastly, some considerations should be made in understanding the use of compounded atropine. In the US, low-dose atropine must be obtained from compounding pharmacies, which often produce the product in small batches and aren’t held to the same regulations and testing standards as commercial FDA-approved products. A survey of different compounding pharmacies across the US revealed a large variety of production methods, ingredients and storage recommendations.28 Further evaluation of some of these products showed potency and stability variation, which in turn may affect myopia management efficacy.29 Inconsistencies of atropine product may make it harder to evaluate efficacy, particularly with such low doses.
Conclusion. Strong emphasis was placed on compliance and continued use of nightly ortho-K lens wear. Atropine was also added to this patient’s therapy. Lastly, more frequent and continuous monitoring of compliance was added. The best modality for an individual child is the one that they will use, as compliance is key to effective treatment.
 |
|
Fig. 4. Axial length progression over time of the right (blue) and left (red) eyes. Soft multifocal lens wear was initiated in August 2017. After poor compliance, the patient was switched to ortho-K in October 2018. Patient reported inconsistent lens wear and low-dose atropine was added in October 2019. Click image to enlarge. |
Takeaways
Each of these cases presents unique challenges and requires customized approaches based on the individual patient data, clinical evidence and practical considerations. By staying up to date on the latest research and clinical strategies, practitioners can effectively manage myopia progression and enhance patient outcomes.
Dr. Tomiyama is an Assistant Professor of Optometry at Marshall B. Ketchum University. She completed a Cornea and Contact Lens Residency at the University of Houston College of Optometry, during which she was introduced to clinical research and decided to pursue a MS, then PhD in Physiological Optics. In her current role, Dr. Tomiyama teaches in the basic science and contact lens curriculum and serves as a clinical attending in the Stein Family Cornea & Contact Lens Center. She has a passion for myopia management and spearheads the Myopia Management Service at the university. Her research areas of interest are myopia, optics, contact lenses and astigmatic corrections. Dr. Tomiyama is a fellow of the American Academy of Optometry and a two-time Ezell Fellowship recipient. She is a consultant for Euclid and Vyluma and a researcher for CooperVision.
1. Flitcroft DI, He M, Jonas JB, et al. IMI – defining and classifying myopia: a proposed set of standards for clinical and epidemiologic studies. Invest Ophthalmol Vis Sci. 2019;60(3):M20-30. 2. Zadnik K, Sinnott LT, Cotter SA, et al. Prediction of juvenile-onset myopia. JAMA Ophthalmol. 2015;133(6):683-9. 3. Bullimore MA, Brennan NA. Myopia: an ounce of prevention is worth a pound of cure. Ophthalmic Physiol Opt. 2023;43(1):116-21. 4. Mutti DO, Mitchell GL, Moeschberger ML, Jones LA, Zadnik K. Parental myopia, near work, school achievement, and children’s refractive error. Invest Ophthalmol Vis Sci. 2002;43(12):3633-40. 5. Xiong S, Sankaridurg P, Naduvilath T, et al. Time spent in outdoor activities in relation to myopia prevention and control: a meta-analysis and systematic review. Acta Ophthalmol. 2017;95(6):551-66. 6. Ip JM, Saw SM, Rose KA, et al. Role of near work in myopia: findings in a sample of Australian school children. Invest Ophthalmol Vis Sci. 2008;49(7):2903-10. 7. Mutti DO, Hayes JR, Mitchell GL, et al. Refractive error, axial length, and relative peripheral refractive error before and after the onset of myopia. Invest Ophthalmol Vis Sci. 2007;48(6):2510-9. 8. Yam JC, Zhang XJ, Zhang Y, et al. Effect of low-concentration atropine eyedrops vs. placebo on myopia incidence in children: the LAMP2 randomized clinical trial. JAMA. 2023;329(6):472-81. 9. Wang W, Zhang F, Yu S, et al. Prevention of myopia shift and myopia onset using 0.01% atropine in premyopic children — a prospective, randomized, double-masked and crossover trial. Eur J Pediatr. 2023;182(6):2597-606. 10. Fang PC, Chung MY, Yu HJ, Wu PC. Prevention of myopia onset with 0.025% atropine in premyopic children. J Ocul Pharmacol Ther. 2010;26(4):341-5. 11. Tsai DC. Early intervention for premyopic children. National Library of Medicine. clinicaltrials.gov/study/NCT06200194. Last updated January 19, 2024. Accessed July 14, 2024. 12. COMET Group. Myopia stabilization and associated factors among participants in the Correction of Myopia Evaluation Trial (COMET). Invest Ophthalmol Vis Sci. 2013;54(13):7871-84. 13. Guo B, Cheung SW, Kojima R, Cho P. One-year results of the Variation of Orthokeratology Lens Treatment Zone (VOLTZ) Study: a prospective randomised clinical trial. Ophthalmic Physiol Opt. 2021;41(4):702-14. 14. Wan K, Lau JKK, Cheung SW, Cho P. Orthokeratology with increased compression factor (OKIC): study design and preliminary results. BMJ Open Ophthalmol. 2020;5(1):e000345. 15. He Y, Liu L, Vincent SJ. Compression factor and visual performance in adults treated with orthokeratology. Eye Contact Lens. 2021;47(7):413-9. 16. Cho P, Cheung SW, Edwards M. The Longitudinal Orthokeratology Research in Children (LORIC) in Hong Kong: a pilot study on refractive changes and myopic control. Curr Eye Res. 2005;30(1):71-80. 17. Kakita T, Hiraoka T, Oshika T. Influence of overnight orthokeratology on axial elongation in childhood myopia. Invest Ophthalmol Vis Sci. 2011;52(5):2170-4. 18. Charm J, Cho P. High myopia–partial reduction ortho-k: a two-year randomized study. Optom Vis Sci. 2013;90(6):530-9. 19. Xu S, Li Z, Zhao W, et al. Effect of atropine, orthokeratology and combined treatments for myopia control: a two-year stratified randomised clinical trial. Br J Ophthalmol. 2023;107(12):1812-7. 20. Mountford J, Pesudovs K. An analysis of the astigmatic changes induced by accelerated orthokeratology. Clin Exp Optom. 2002;85(5):284-93. 21. Tomiyama ES, Berntsen DA, Richdale K. Peripheral refraction with toric orthokeratology and soft toric multifocal contact lenses in myopic astigmatic eyes. Invest Opthalmol Vis Sci. 2022;63(8):10. 22. Tomiyama ES, Hu C, Marsack JD, Richdale K. Greater higher order aberrations induced by toric orthokeratology versus soft toric multifocal contact lens wear. Ophthalmic Physiol Opt. 2021;41(4):726-35. 23. Tomiyama ES, Richdale K. Clinical outcomes of a randomized trial with contact lenses for astigmatic myopia management. Optom Vis Sci. 2023;100(1):9-16. 24. Tan Q, Ng AL, Choy BN, et al. One-year results of 0.01% atropine with orthokeratology (AOK) study: a randomised clinical trial. Ophthalmic Physiol Opt. 2020;40(5):557-66. 25. Kinoshita N, Konno Y, Hamada N, et al. Additive effects of orthokeratology and atropine 0.01% ophthalmic solution in slowing axial elongation in children with myopia: first year results. Jpn J Ophthalmol. 2018;62(5):544-53. 26. Chen Z, Zhou J, Xue F, Qu X, Zhou X. Two-year add-on effect of using low-concentration atropine in poor responders of orthokeratology in myopic children. Br J Ophthalmol. 2022;106(8):1069-72. 27. Jones JH, Mutti DO, Jones-Jordan LA, Walline JJ. Effect of combining 0.01% atropine with soft multifocal contact lenses on myopia progression in children. Optom Vis Sci. 2022;99(5):434-42. 28. Richdale K, Tomiyama ES, Novack GD, Bullimore MA. Compounding of low-concentration atropine for myopia control. Eye Contact Lens. 2022;48(12):489-92. 29. Richdale K, Skidmore KV, Tomiyama ES, Bullimore MA. Compounded 0.01% atropine-what’s in the bottle? Eye Contact Lens. 2023;49(6):219-23. |
