 |
Optometrists are becoming increasingly involved in working alongside ophthalmology in providing postoperative care. This case highlights issues that can arise when the surgeon is not promptly available to care for post-op complications that might require additional surgical intervention. In this case, the optometrist followed standard of care in treatment of a postoperative LASIK complication but the patient now has mildly reduced vision in one eye and blames the optometrist for what he deems to be a poor outcome.
Case
A 35-year-old male presented to an optometrist (working alongside ophthalmologists at a refractive surgery center) one day after LASIK OU complaining of a “grainy feeling” in his eyes and eye pain OD>OS. Unaided VA was 20/25 OD and 20/30-1 OS with no abnormal findings present on slit lamp exam. Pred Forte QID OU was prescribed and the patient was told to continue artificial tears as needed and to follow up in three days. The patient followed up as indicated three days later and vision had improved to 20/20 OD and OS; however, diffuse lamellar keratitis (DLK) was noted OD>OS (graded 3+ OD, 2+ OS).
The optometrist attempted to contact the surgeon while the patient was still in the office but could not get an answer. The optometrist instructed the patient to increase use of the steroid drops to every hour OU and also prescribed oral methylprednisone. The optometrist noted that he later that same day had spoken to the surgeon, who agreed with this plan, but the surgeon did not indicate any need to examine the patient himself. Per the records, the surgeon told the optometrist if there was no clumping of cells anywhere and vision was 20/20, the patient did not need to be seen by the surgeon that day. The patient was told to follow up one day later. The patient did return the next day, the vision remained 20/20 OD and OS and they were told to continue the treatment plan.
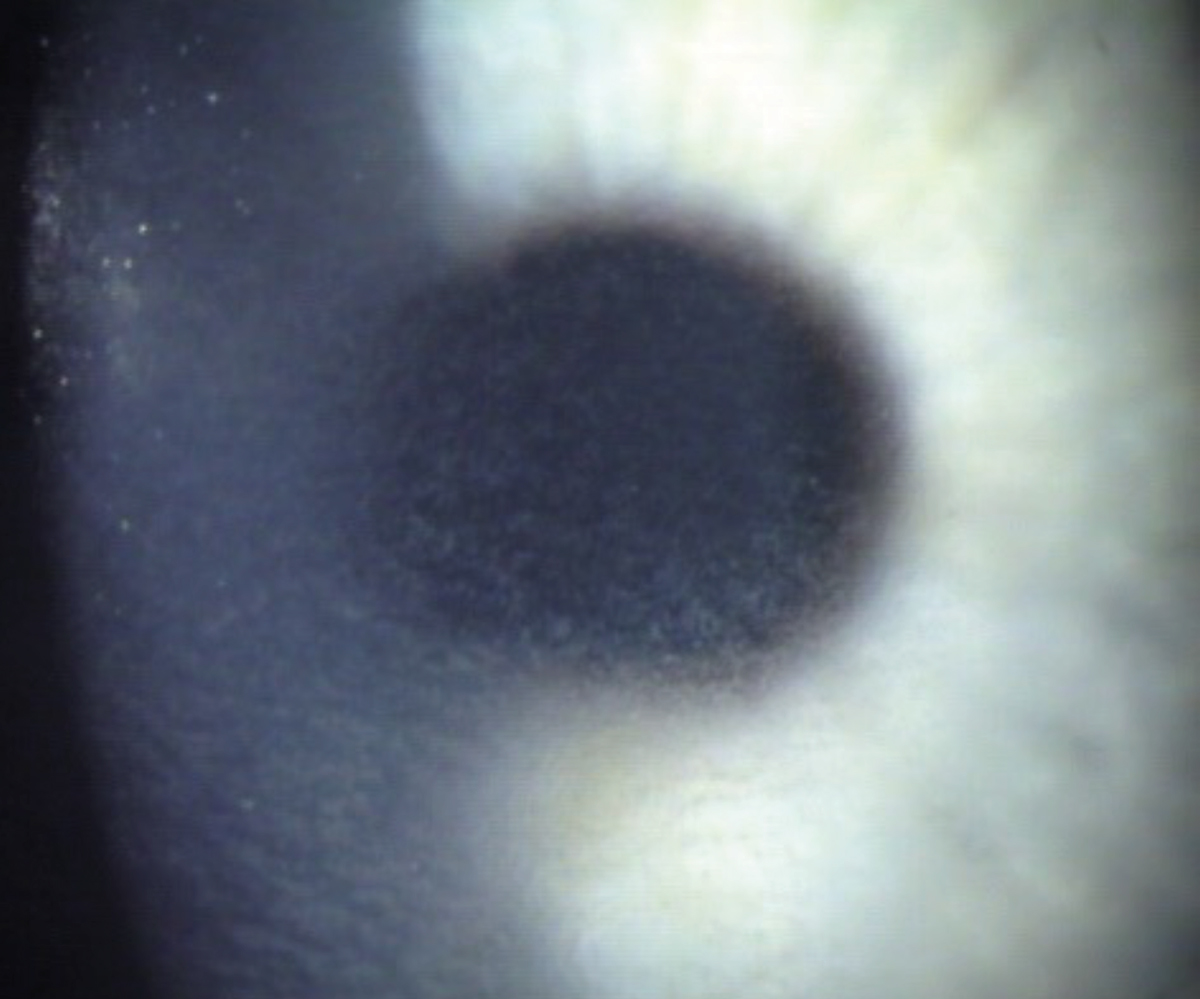 |
| Grade 2 DLK reveals diffuse spreading of inflammatory cells over the entire cornea. In grade 1, the cells are limited to the peripheral cornea. This appearance was termed “sands of Sahara” in older literature. Photo: Jim Thimons, OD, Eric Donnenfeld, MD. Click image to enlarge. |
The following day, the patient returned and was now examined by the surgeon. The vision was now reduced to 20/60- OD, 20/20- OS. Per the patient, the surgeon was visibly alarmed by the corneal status at this visit and reported that he had not been advised on the severity of the condition. He recommended and performed a flap lift and irrigation OU. Signed informed consent was obtained as it was prior to the LASIK procedure. The next day, vision had improved to 20/40 OD and remained 20/20 OS. The patient continued the oral and topical steroid with taper as scheduled.
At the most recent eye exam about one year later, vision without correction was noted to be 20/30-2 OD, 20/20 OS with subtle subepithelial haze centrally OD. The patient reported no sensitivity to light and no eye pain. Difficulty driving at night secondary to halos in vision was reported and the patient is currently using Restasis (cyclosporine A ophthalmic emulsion 0.05%, Allergan) BID OU and preservative-free artificial tears PRN. The most recent refraction about a year after LASIK was +0.25 OD and plano OS.
You Be the Judge
Considering the facts presented thus far, consider the following questions:
- Did the optometrist properly treat diffuse lamellar keratitis?
- Is the optometrist culpable for malpractice even though his treatment plan was discussed with and recommended by the patient’s surgeon?
- Even though the optometrist attempted to contact the surgeon and did not initially get an answer, should the OD have insisted the patient be seen by the surgeon that day?
- Is the patient’s current vision and visual function reduced enough to significantly impact his quality of life?
- What would a practitioner under like circumstances have done on the first visit?
Our Opinion
One of us (JS) agreed to review the case for the plaintiff’s two attorneys. After reaching an opinion, I requested permission to have the case reviewed entirely independently, and at no additional charge, by a young colleague (DD) who recently graduated number one in her class at SUNY. Neither of us could find any culpability on the part of the OD but both of us were less sure about the role of the surgeon.
Discussion
DLK is a noninfectious complication of refractive surgery occurring early in the postoperative period and affecting 2% to 4% of patients that undergo LASIK surgery.1 Also known as “sands of Sahara” syndrome, it is characterized by fine, white inflammatory infiltrates beneath the corneal flap interface. Patients often complain of pain, foreign body sensation, photophobia and blurry vision.2 It is broken up into four grades. Grade 1 consists of peripheral infiltrates only without central involvement. Grade 2 consists of central involvement, which can begin to affect visual acuity. During grade 3, there can be clumping of cells and permanent corneal scarring, and in grade 4, stromal melting and further corneal scarring occur along with a hyperopic shift.3
The condition typically responds well to steroid treatment. For grades 1 and 2, topical steroids are typically recommended hourly during the day with a steroid ointment at bedtime. It is recommended that the patient is seen 48 hours later for evaluation and to begin tapering. Once DLK reaches the third grade, most surgeons perform irrigation along with steroid treatment, which at this stage may include oral steroids. Early treatment of DLK is imperative in preventing progression to the later stages.
Is the Surgeon Culpable?
It has been suggested that surgical technique can play a role in the development of DLK. Exposure to red blood cells, sponge fibers, debris from surgical instruments, powder from surgical gloves, iatrogenic epithelial defects or meibomian gland secretions can instigate inflammation and play a role in disrupting corneal epithelial cells.4 Contaminated instruments are considered a common cause. Also, in this case the surgeon was given the chance to evaluate the patient sooner and declined. Both arguments could be caused by time constraints, especially in a high-volume practice. Surgeons may take shortcuts that lead to complications and unhappy patients.
 |
|
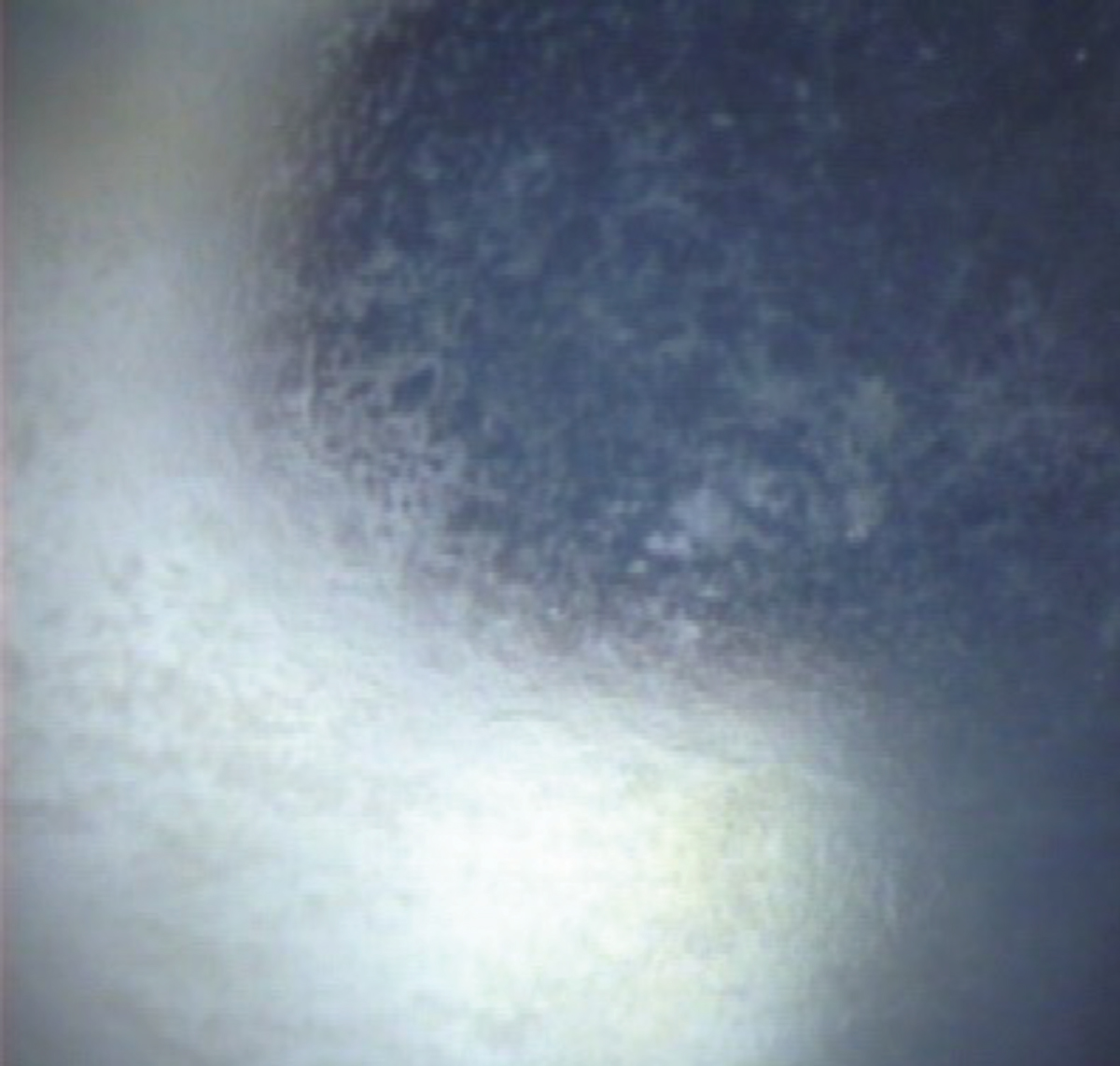
Grade 3 DLK reveals clumped opacities believed to be white blood cells. Photo: Jim Thimons, OD, and Eric Donnenfeld, MD. Click image to enlarge. |
Further Comments
Given the grading of the DLK documented by the optometrist, the treatment regimen of frequent topical steroid along with oral steroids seems to follow the standard of care. While flap irrigation is usually indicated once DLK reaches grade 3, the optometrist relayed his findings to the surgeon, who agreed with the proposed plan at the time and did not feel the need to examine the patient himself that day. The OD continued to follow up with the patient closely throughout the course of treatment.
The optometrist did attempt to contact the surgeon while the patient was present but was unable to. The OD appeared to have accurately staged the severity of the DLK at that visit and relayed those findings to the surgeon (according to the patient, the surgeon seemed “alarmed” and was told he was not advised on the severity of the condition, although grade 3+ DLK is noted by the optometrist in his chart note).
Overall, the patient ended up with 20/30 uncorrected VA OD with mild central subepithelial haze and 20/20 vision OS with no pain. In our opinion, this is unlikely to significantly impact the patient’s visual function and quality of life. Additionally, the patient was informed of potential risks prior to the procedure and signed a detailed informed consent. Patients undergoing LASIK often expect a perfect outcome, but this is not always attainable. Optometrists frequently play a role in refractive surgery postoperative care, and in most cases, referral to the surgeon after noting DLK is typically not deemed necessary, as it usually responds well to steroid therapy.Outcome
I (JS) spoke with the lead attorney and presented my findings and conclusions followed by the independent conclusions reached by my colleague. The attorney was clearly disappointed and also appeared disheartened by the two independent conclusions. The patient has options: either request that his attorneys find another optometrist to review the case or identify another attorney who will then find another OD to review the case and perhaps reach a different conclusion. The patient, through his attorneys, can decide to bring charges against the surgeon. The attorneys will then need to find expert witnesses, other LASIK surgeons, to review the case.
Upon recent request, the patient has graciously given his permission to present this case for educational purposes.
Dr. Doscas graduated from SUNY College of Optometry in 2023. She completed her residency training in primary care optometry and ocular disease at VA Hudson Valley and is currently employed at a private practice in White Plains, NY.
| NOTE: This article is one of a series based on actual lawsuits in which the author served as an expert witness or rendered an expert opinion. These cases are factual, but some details have been altered to preserve confidentiality. The article represents the authors’ opinion of acceptable standards of care and do not give legal or medical advice. Laws, standards and the outcome of cases can vary from place to place. Others’ opinions may differ; we welcome yours. |
Dr. Sherman is a Distinguished Teaching Professor at the SUNY State College of Optometry and editor-in-chief of Retina Revealed at www.retinarevealed.com. During his 52 years at SUNY, Dr. Sherman has published about 750 various manuscripts. He has also served as an expert witness in 400 malpractice cases, approximately equally split between plaintiff and defendant. Dr. Sherman has received support for Retina Revealed from Carl Zeiss Meditec, MacuHealth and Konan.
Dr. Bass is a Distinguished Teaching Professor at the SUNY College of Optometry and is an attending in the Retina Clinic of the University Eye Center. She has served as an expert witness in a significant number of malpractice cases, the majority in support of the defendant. She serves as a consultant for ProQR Therapeutics.
1. Azar DT, Koch DD. LASIK: Fundamentals, Surgical Techniques and Complications. New York, NY: Marcel Dekker; 2003. 2. Balestrazzi A, Balestrazzi A, Giannico MI, et al. Diagnosis, clinical trend and treatment of diffuse lamellar keratitis after femtosecond laser-assisted in situ keratomileusis: a case report. Case Rep Ophthalmol. 2018;9(3):457-64. 3. Smith RJ, Maloney RK. Diffuse lamellar keratitis. A new syndrome in lamellar refractive surgery. Ophthalmology. 1998;105(9):1721-6. 4. Warren N, Feldman BH, Buckner B, et al. Diffuse lamellar keratitis. EyeWiki. eyewiki.org/diffuse_lamellar_keratitis. Updated June 23, 2024. Accessed September 23, 2024. |
