 |
“Doc, I think my cataracts have come back.” We have all heard that statement before, especially after cataract surgery. Yttrium aluminum garnet (YAG) laser capsulotomy, a procedure that came about in the late 1970s, is an in-office intervention that is being performed more and more by optometrists as scope of practice advances across the nation. It is one of the most rewarding procedures eyecare providers perform and likely represents the number one laser procedure that optometrists have been completing over the past decade. Here are the nuts and bolts of the procedure.
Indications and Contraindications
Knowing when to do vs. when not to do a procedure is critical for any treating doctor. YAG laser capsulotomy is indicated following cataract surgery when posterior capsular opacification (PCO) has caused vision to fall to the point where it affects activities of daily living. Generally, patients often have visual acuities of 20/25, 20/30 or worse, but glare symptoms or other affected activities of daily living may drive a patient to seek care before vision has fallen on the Snellen acuity chart.
Contraindications include active inflammation within the eye, significant corneal or other media opacities that affect viewing of the posterior capsule and a patient that is unable to hold steady or fixate appropriately to undergo the procedure. Any active retinal conditions—such as macular edema, macular hole or vitreomacular traction, among others—should be properly assessed. Also, determine whether a retinal consult should be obtained before performing the YAG capsulotomy, as there is the rare risk of worsening macular or retinal conditions when a laser procedure is performed inside the eye. In my experience, the report back from the retina specialist quite often includes a statement like “clear up and open the posterior capsule so I can better assess the retinal condition.” Regardless, caution is always recommended especially in early cases.
 |
|
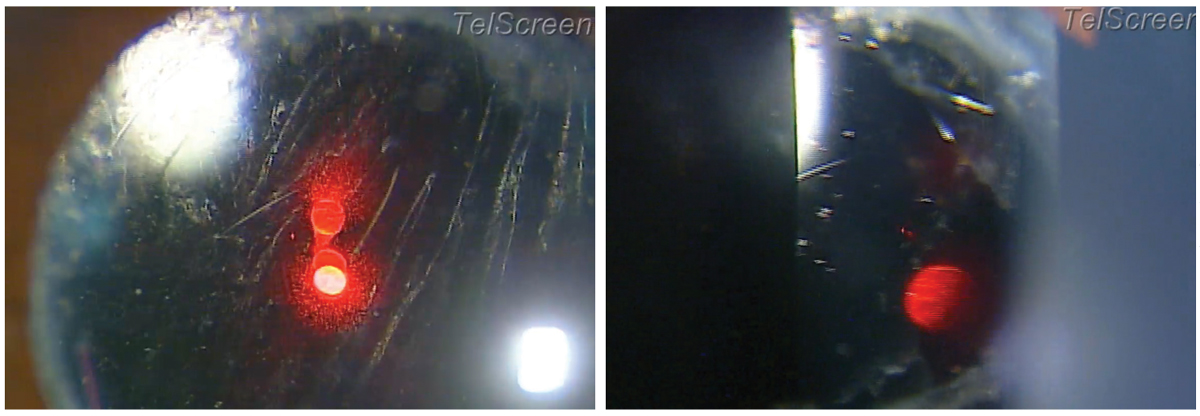
Fig. 1. Peripheral lens pit seen while doing a YAG capsulotomy. This indicates laser energy was focused too far anteriorly. Acuity was not affected due to the peripheral location. Click image to enlarge. |
Potential Complications
Fortunately, these are rare with YAG laser capsulotomy. Rare complications, including the approximate rate of occurrence based on the literature and clinical experience, as well as proper management if the complication occurs, include:1-5
- Intraocular pressure (IOP) spike, 5% to 15%. The literature shows an IOP spike rate of approximately 10% following capsulotomy; however, with pre- and postoperative in-office use of brimonidine, clinical experience shows the rate of IOP spike to be in the range of 1% to 5%.
- Inflammation/uveitis, 1% to 10%. The rate of a clinically significant iritis following a YAG capsulotomy is very low. The more energy used for the procedure, the higher the likelihood of an inflammatory response. This can be controlled in the postoperative period with a topical steroid if needed.
- Intraocular (IOL) lens pitting, 8% to 33%. Proper focus of the laser and correct offset settings will minimize this potential complication (Figure 1).
- Floaters, 10% to 20%. Based on clinical experience. A temporary increase in floaters is fairly common after a YAG; however, the floaters most often subside in a matter of days to weeks.
- Cystoid macular edema, 0% to 2.9%. Very rare complication which can be treated with topical steroid and/or topical non-steroidal drops.
- Retinal tears/breaks/detachments, 0% to 2.3%. Very rare complication that can occur anywhere from days to a year plus following a YAG capsulotomy. Proper diagnosis and prompt referral to a retinal specialist is warranted.
 |
|
Fig. 2. Preoperative appearance of a standard grade 2 PCO (left), as well as the appearance of the capsule at the end of the procedure (right). Notice the nicely opened capsule. Visual acuity improved from 20/40 to 20/20. Photo: NSU Oklahoma College of Optometry. Click image to enlarge. |
Procedural Technique
Let’s review how to perform YAG capsulotomy.
1. Complete a thorough dilated fundus exam including posterior pole and peripheral retinal evaluation.
2. Preoperative drops include topical ophthalmic brimonidine one to two drops in the eye to be treated 10 to 15 minutes prior to the procedure to help blunt the risk of an IOP spike, along with topical ophthalmic proparacaine immediately prior to the procedure in both eyes to eliminate a blink reflex. A consent form should be reviewed and signed before every procedure.
3. The use of a YAG capsulotomy laser lens is physician preference, with ophthalmology surveys showing approximately half of ophthalmologists prefer the use of a laser lens, while the other half prefers to do the procedure without a laser lens. I prefer to use a laser lens to give control and stability of the eye and provide a better view of the posterior capsule, especially if any ocular surface disease is present. Cushioning solution, such as Genteal gel (hypromellose 0.3%, Novartis), is necessary if a laser lens is used. Downsides of using a laser lens include another step that needs to be done (putting the laser lens on the eye), as well as another interface for glare to develop along with bubbles to form in the cushioning solution.
4. Laser settings are critical to properly perform any laser procedure. Three main settings can be adjusted by the physician as the YAG laser is being set up to perform a YAG capsulotomy.
Energy (in mJ). Typically, energy setting varies based on physician preference and thickness and density of the PCO. It is recommended to start in the range of 1.5mJ to 2.0mJ. I use 1.6mJ for a standard grade 1 to 2+ PCO.
Offset (in microns). Using a posterior offset is important to minimize the likelihood of lens pitting during the procedure. The recommendation is somewhere between 150µm and 300µm of posterior offset when performing a standard YAG laser posterior capsulotomy. This setting is again a physician preference. The type of IOL material can also play a role in how much offset is used, with clinical experience showing that silicone IOLs (such as the light-adjustable lens) are perhaps slightly more prone to pitting, and therefore some recommend increasing the offset by an extra 50µm to 100µm whenever treating silicone IOLs.
Burst mode (single, double or triple shot). Typically, YAG capsulotomies are performed on single shot mode as that is all that is needed. Double shot or triple shot are typically reserved for YAG laser peripheral iridotomies in darker irises.
One critical note: a timeout should be performed by the doctor and one other individual (e.g., staff member, student, resident) after the laser settings have been dialed in and before the procedure begins to double check and ensure that the right laser mode/setting is selected along with the correct and intended energy level, offset and burst mode. A timeout should be performed prior to every procedure.
5. The YAG laser capsulotomy pattern or technique is also dependent on physician preference. YAG capsulotomy techniques or patterns include cruciate/modified cruciate (cross-like), circular, hinge/horseshoe, spiral, star and postage stamp.
Of these types of patterns, the cruciate/cross-like and circular are the most common and most popular among treating eyecare providers. Ophthalmology surveys show that the cruciate technique is more than double the next most popular pattern, which is the circular technique. One study reported that “Both the cross-like and circular YAG capsulotomy techniques induce similar visual and IOP changes. The circular technique is associated with a higher amount of energy used and more floater symptoms.”6
 |
|
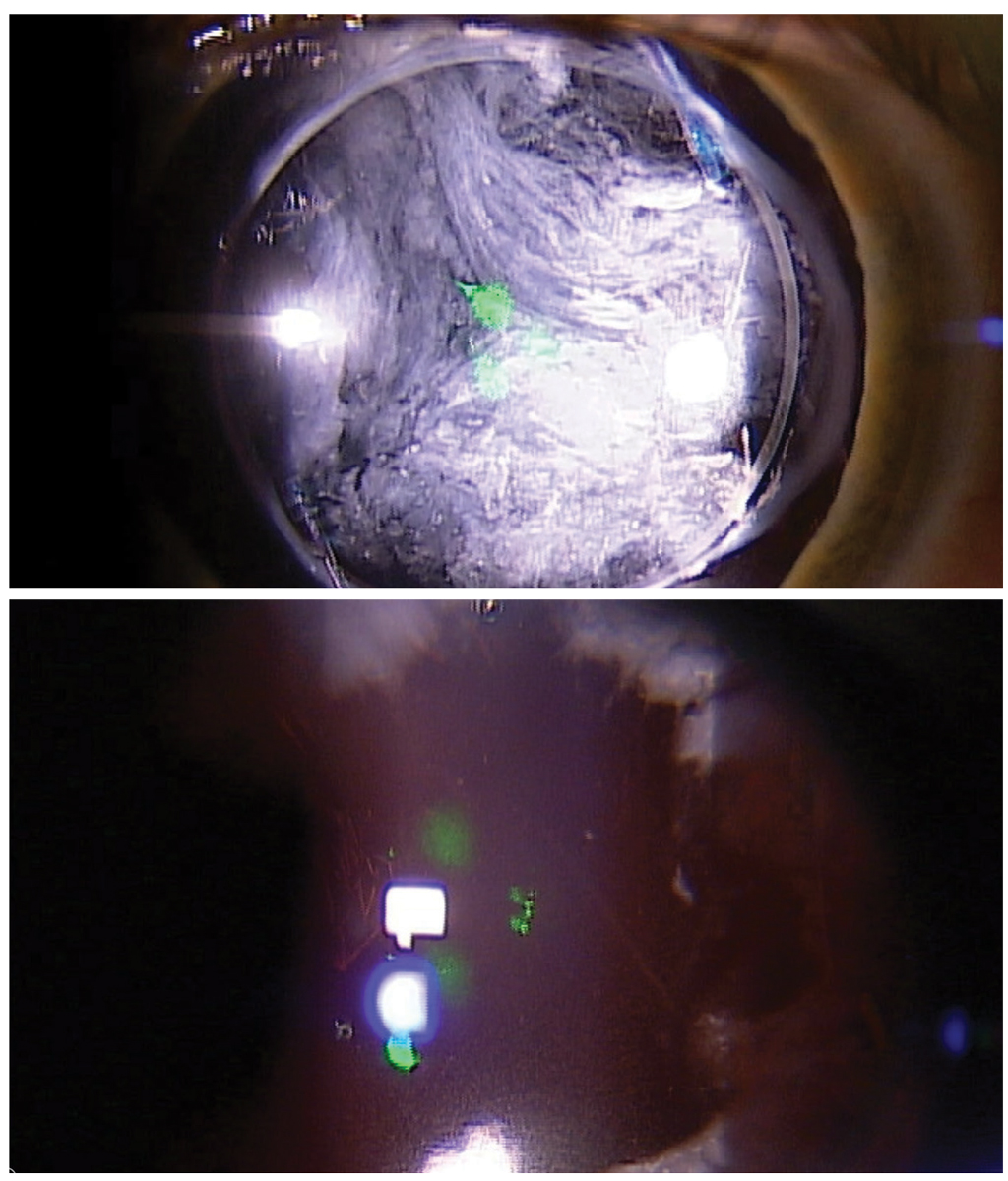
Fig. 3. Preoperative appearance of a significant grade 4 PCO (top), as well as the appearance of the capsule at the end of the procedure (bottom). Visual acuity improved from hand motion to 20/30. Click image to enlarge. |
I prefer the cross-like pattern starting near the top center of the PCO and working my way straight down the vertical meridian. Once the vertical meridian is complete and open, the horizontal part of the cross pattern is done, starting near the center and working outwards towards the periphery in both the left and right directions (Figures 2 and 3). If the capsule is agreeable, the four flaps that are formed from the cross-like technique will fold back on their own instantaneously and won’t require many further shots to move the flaps away from the visual axis. Often, the flaps won’t fold back on their own instantaneously, and a few more shots at each flap will be required to assist each flap in folding back and out of the visual axis.
6. The typical number of shots for a YAG capsulotomy is often somewhere between 20 and 60, although some cases require more or fewer shots depending on the thickness and density of the PCO. Our record is a seven-shot capsulotomy by Greg O’Brien, OD, during his residency approximately 15 years ago. Beat that!
7. Once the YAG capsulotomy is complete, one to two drops of topical ophthalmic brimonidine are instilled in the treated eye again to control for any postoperative IOP spike. We check the patient’s IOP 30 to 60 minutes after the procedure, and if the IOP is similar to preoperative levels, we release the patient until the one-week follow-up visit. We currently do not put the patient on a postoperative steroid eye drop; however, depending on practitioner preference and number of shots needed to clear the PCO, a topical steroid two to four times daily for three to five days could be prescribed.
Takeaways
YAG laser capsulotomy is almost always a quick in-office procedure that greatly helps patients see better and improve on their activities of daily living. The literature has shown that YAG laser capsulotomies are effective treatments to improve patient vision that can be safely and effectively performed by ODs.7 Optometrists nationwide are encouraged to adopt this procedure if scope of practice allows in your state or be very familiar with the comanagement aspects of the procedure if current scope does not allow it. YAG laser capsulotomy is one of the most rewarding procedures for eye doctors, and, most importantly, one of the most immediately gratifying and helpful procedures for patients.
Dr. Lighthizer is the associate dean, director of continuing education and chief of specialty care clinics at the NSU Oklahoma College of Optometry. He is a founding member and immediate past president of the Intrepid Eye Society. Dr. Lighthizer’s full disclosure list can be found here.
1. Karahan E, Tuncer I, Zengin MO. The effect of ND: YAG laser posterior capsulotomy size on refraction, intraocular pressure and macular thickness. J Ophthalmol. 2014;2014:846385. 2. Ge J, Wand M, Chiang R, et al. Long-term effect of Nd:YAG laser posterior capsulotomy on intraocular pressure. Arch Ophthalmol. 2000;118(10):1334-7. 3. Steinert RF. Neodymium:yttrium-aluminium-garnet laser posterior capsulotomy. In: Gabbedy R, Mortimer A, eds. Cataract Surgery. 3rd ed. Philadelphia, PA: Elsevier Inc; 2010:617-29. 4. Karahan E, Er D, Kaynak S. An overview of Nd:YAG laser capsulotomy. Med Hypothesis Discov Innov Ophthalmol. 2014;3(2):45-50. 5. Bhargava R, Kumar P, Sharma SK, Kaur A. A randomized controlled trial of peeling and aspiration of Elschnig pearls and neodymium: yttrium-aluminium-garnet laser capsulotomy. Int J Ophthalmol. 2015;8(3):590-6. 6. Kara N, Evcimen Y, Kirik F, et al. Comparison of two laser capsulotomy techniques: cruciate vs. circular. Semin Ophthalmol. 2014;29(3):151-5. 7. Lighthizer N, Johnson S, Holthaus J, et al. Nd:YAG laser capsulotomy: efficacy and outcomes performed by optometrists. Optom Vis Sci. 2023;100(10):665-6. |
