25th Annual Dry Eye ReportThe most commonly encountered ocular condition enters the spotlight this month. Inside the May 2024 issue of Review of Optometry, get the scoop on omega fatty acids for dry eye, learn how to match dry eye patients to treatments and find a step-by-step guide to managing OSD. Check out the other dry eye-themed articles featured in this issue:
|
Dry eye syndrome is one of the most prevalent ocular conditions, affecting people across age groups and lifestyles. Its commonality is a testament to the evolving landscape of modern living as well as an important reminder of the intricate balance required for optimal ocular health. Experiencing the digital era’s relentless screen time demands and other environmental stressors, the discomfort of dry eyes has become more than just an inconvenience—it has evolved into a persistent challenge that demands timely chronic treatment.
To manage the condition effectively, traditional approaches such as artificial tears and prescription medications often take center stage; however, navigating the systemic underpinnings of ocular health reveals an obvious connection between dietary choices and the well-being of our eyes. Many practitioners have long considered nutritional supplements such as omega-3 fatty acids (O3FAs) to be a viable aid not only in management of dry eye but prevention as well. This conventional wisdom has been challenged in recent years; however, leaving clinicians with some uncertainty. Let’s delve into the topic of support for—and skepticism of—omega fatty acid use in dry eye.
Dietary Significance
Fatty acids are an essential building block to maintain proper human function. O3FAs comprise alpha-linolenic acid, eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). Omega-6 FAs (O6FAs), which conversely possess proinflammatory properties, consist of linoleic acid, gamma-linolenic acid, dihomogamma-linolenic acid and arachidonic acid.1,2
It is suspected that humans evolved to intake a ratio of O6FAs to O3FAs close to 1:1. The Western diet typically maintains a ratio around 15:1, resulting in an excessive proinflammatory environment.3 This skewed ratio is believed to contribute significantly to the elevated prevalence observed of cardiovascular diseases, autoimmune conditions, cancers and other inflammatory conditions within the Western population.4
It is important to convey to patients the dietary need for consuming foods rich in O3FAs. Widely available options include salmon, herring, tuna, sardines, flaxseed oil, edamame, walnuts, soybeans and fortified foods such as eggs, yogurt, juices, milk and infant formulas.5-7 If patients cannot achieve a healthy O3FA intake, a supplement may be advised.
Omega-3 and omega-6 are essential fatty acids (EFAs) needed to produce eicosanoids, a class of hormone-like lipids that help regulate inflammation and provide local neutrophil migration. There are multiple types of eicosanoids: prostaglandins, thromboxanes and leukotrienes.8 O3FAs and O6FAs physiologically have different purposes. O3FAs have anti-inflammatory and anticoagulant properties, whereas O6FAs promote inflammation and platelet aggregation.5
 |
|
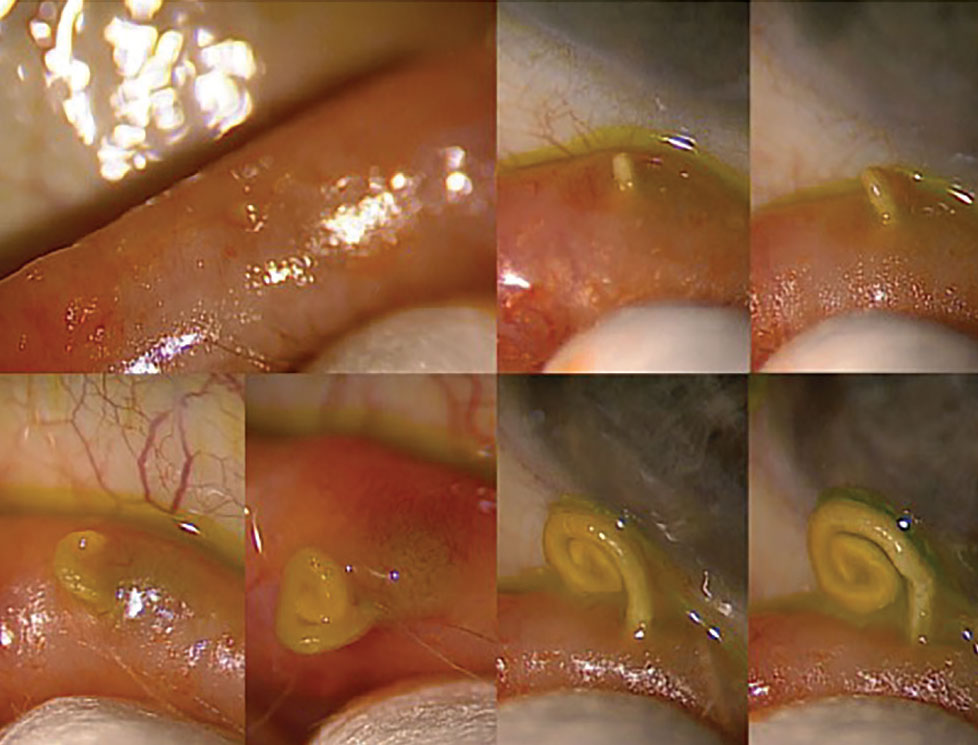
Expression of a gland experiencing obstruction. Click image to enlarge. |
O3FAs may be anti-inflammatory through numerous mechanisms. O3FAs and O6FAs compete for the same enzyme to produce their respective eicosanoids. Note that eicosanoids are local signaling molecules needed to regulate different homeostatic processes. O3FAs tend to produce anti-inflammatory eicosanoids, whereas O6FAs tend to produce inflammatory eicosanoids. There is some evidence linking O3FAs to downregulating the production of inflammatory signaling molecules such as cytokines and chemokines.9 These molecules are needed for homeostasis, but an overproliferation can lead to a chronic inflammatory environment. O3FAs also interact with genes influencing the production of inflammatory proteins.6
Other than producing inflammatory eicosanoids and competitively inhibiting O3FA metabolism, O6FAs are also proinflammatory through cellular signaling. O6FAs can interact with cellular receptors to enhance production of inflammatory proteins like cytokines.
Resolvins are a group of O3FA metabolite molecules present in the liver, lungs and eyes. These molecules possess special properties for controlling the length and density of inflammation.3 They have shown positive effects on goblet cell preservation, proper tear secretion and reduction of antigen-presenting cells into the cornea.10
Link to Dry Eye
Because of the well-known anti-inflammatory effect of O3FAs, it is accepted by many that an oral supplement may provide a therapeutic effect for patients suffering from dry eye. O6FAs and O3FAs compete for the same enzyme (desaturase) that allows for their digestion. Breakdown of these EFAs presents with their respective inflammatory or noninflammatory effects.11,12 This leads to two theories for why O3FAs are beneficial. One is that O3FAs compete with O6FAs, allowing for competitive inhibition. An alternative theory stems from evidence suggesting that O3FA supplementation can impact meibum composition, potentially aiding in the prevention and treatment of meibomian gland dysfunction.13
 |
|
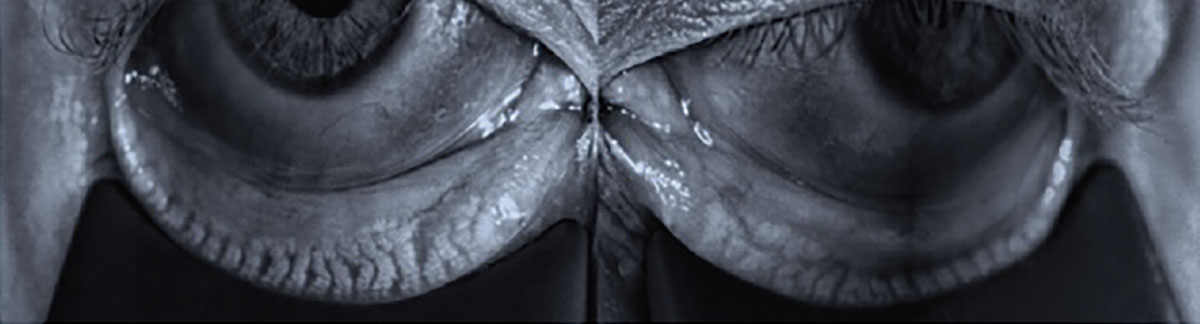
Meibography revealing characteristic signs of meibomian gland dysfunction: gland loss, truncation and tortuosity. Click image to enlarge. |
One study analyzed meibum composition using a technique called high-pressure liquid chromatography, focusing on the peak profiles of polar lipids in patients with Sjögren's syndrome. Findings revealed patients with higher O3FA intake exhibited more single peaks as opposed to multiple peaks in their meibum composition. A single peak of polar lipids suggests the meibum is composed of one distinct type or pattern of polar lipids, whereas multiple peaks indicate a variety of polar lipid types—the latter suggesting less homogeneity in the lipid profile.14 Lack of homogeneity might affect tear film stability, and if the tears' lipid layer is composed of a variety of polar lipids rather than a more uniformed composition, it might be less effective in preventing tear evaporation.
Controversially, the Dry Eye Assessment and Management (DREAM) study, conducted by the National Institute of Health, was released in 2019 and concluded O3FAs serve no benefit over the placebo of refined olive oil within a real world setting.15 This study and its preliminary findings have provided room for clinicians to question whether to prescribe O3FAs to their dry eye patients. The study used olive oil, which is primarily n-9 oleic acid, as the placebo. Olive oil has been a placebo used in other clinical studies as well, but it does bring its own criticism. Oleic acid is thought to possess anti-inflammatory properties similar to O3FAs.16 Subsequently, the DREAM study may have displayed the benefit of olive oil and other types of fats rather than proving that O3FAs are not beneficial for dry eye patients.
The study was also conducted in a real world setting, allowing for influences from factors that were not controlled (e.g., other treatments, diet). A knee-jerk reaction to the study may cause some clinicians to overlook a great natural tool. Do note that this is just one study; more and similar studies are needed to gain a better idea regarding the precision of the results.
In contradistinction to the DREAM study's results, several studies have demonstrated benefits of omega EFAs in treating dry eye. A cross-sectional study using questionnaire-based data revealed a ratio of O6FA to O3FA greater than 15:1 was associated with a twofold higher prevalence of dry eye syndrome. Furthermore, women with greater O3FA intake exhibited reduced syndrome risk.17 In a separate placebo-controlled study spanning 12 weeks, those taking O3FAs showed improvements in dry eye signs and symptoms; these included increased tear break-up time (TBUT), decreased ocular surface disease index score and reduced matrix metalloproteinase-9 positivity.18 Yet another randomized, controlled study saw symptom improvement, reduced osmolarity, increased Schirmer test scores, improved TBUT and increased goblet cell density among patients taking omega EFAs.19
 |
|
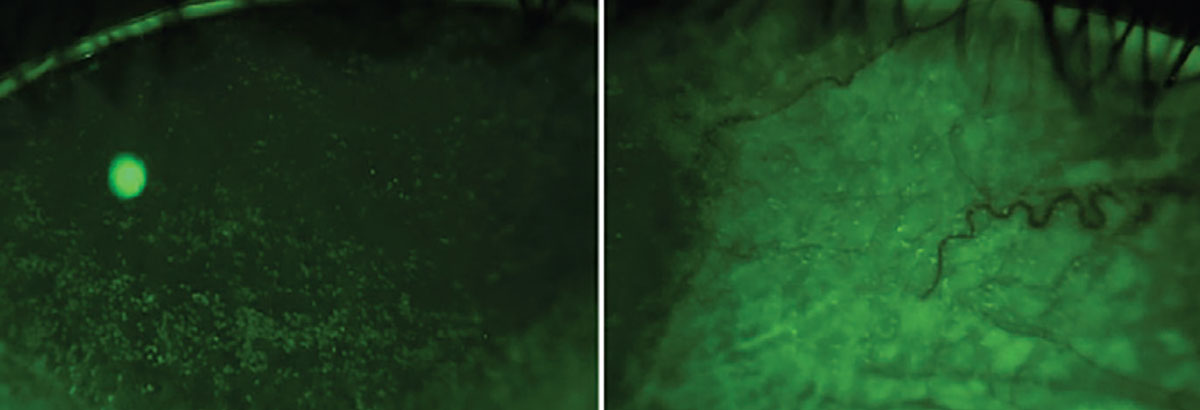
Corneal and conjunctival staining can serve as indicators of a patient's ocular dryness and the specific type of dry eye they may be experiencing. Click image to enlarge. |
Taken together, these studies suggest an improvement across all three tear layers upon O3FA use. Given the substantial body of published clinical research, it becomes challenging to refute the therapeutic advantages of O3FAs when addressing dry eye.
Clinical Use
When contemplating timing and dosage of an O3FA recommendation, it is crucial to consider an individual’s needs. As discussed by the studies in the previous section, O3FAs have demonstrated benefits across all facets of dry eye. Therefore, it is advisable to introduce omega fatty acid supplementation early in the treatment paradigm. Dosages ranging from 1,000mg to 3,000mg of O3FA (EPA/DHA) per day are commonly prescribed for dry eye, reflecting a spectrum of patient needs and clinical considerations. One study concluded a dosage of 1,000mg of O3FA once daily may not be sufficient to yield therapeutic benefits, suggesting instead an intake of 2,000mg or greater to achieve therapeutic concentrations.20
The FDA has classified the acceptable daily intake of O3FAs to be up to 3,000mg per day with physician monitoring.9 Consequently, any dosage exceeding 3,000mg should be prescribed with caution, considering both individual patients’ needs and heightened risk of bleeding and side effects from O3FA.
It is imperative to educate patients that the adjustment of serum O3FA levels can span several months, so symptoms may not improve immediately. Clinicians have access to convenient in-office or home tests provided by third party companies such as OmegaQuant, Lipid Technologies and Carlson Labs, enabling them to conduct quantitative analyses and monitor patients’ omega EFA levels. By integrating these easy-to-use testing options into their practices, clinicians can obtain valuable insights into an individual patient's nutritional status, thereby facilitating targeted interventions and personalized treatment plans.
 |
|
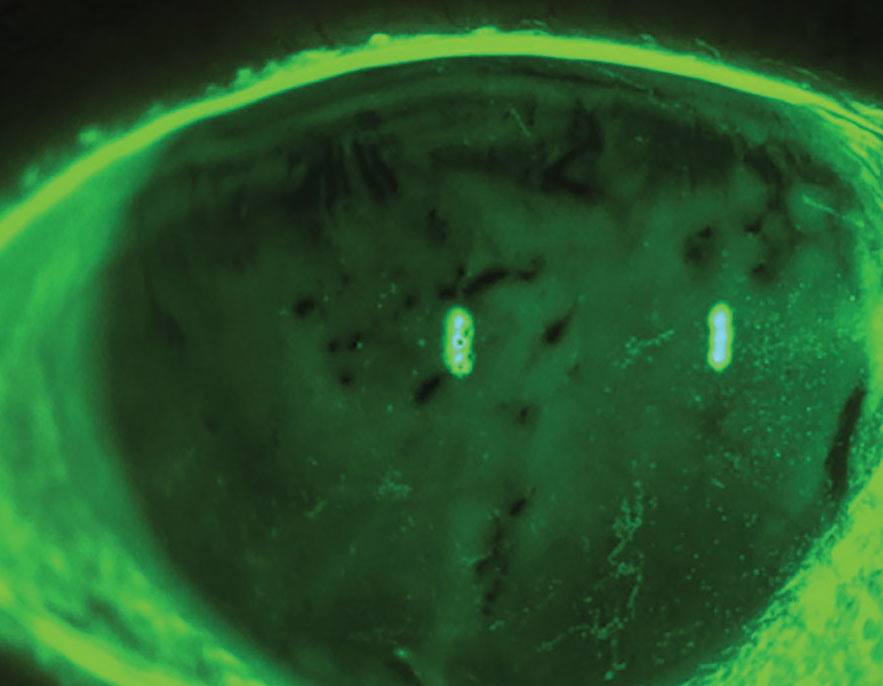
Evaporative dry eye syndrome with reduced tear break-up time and punctate epithelial erosions. Many studies demonstrate O3FAs may help with mitigating signs and/or symptoms. Photo: Luis Rojas, OD. Click image to enlarge. |
It is the prescriber’s responsibility to educate patients in how to select and handle the supplement. Although the intervention is quite safe, the patient should be educated on associated side effects of the supplement. These may include dyspepsia, diarrhea, gas, nausea, fishy taste and arthralgia.21-23 These side effects can be reduced if the supplement is taken with food. It is recommended to stay with brands that conduct testing for the purity of their product. Certain brands available in the US market, including but not limited to Nordic Naturals, Nature Made, Nature Bounty and Sundown, undergo third-party quality testing to ensure their products meet stringent quality standards. The product should be kept in its container and away from light and highly heated environments to reduce oxidation.
Along with its anti-inflammatory properties, O3FAs are also a natural anticoagulant.24 When prescribing them to patients who are already on antiplatelet or anticoagulant medications or who have hemophilia, do so with caution. Always consider consulting the patient’s primary physician if necessary.
Along with taking an oral supplementation, patients may also have access to topical eye drops containing O3FAs specifically derived from flaxseed oil. There have only been limited studies exploring the use of O3FAs in a topical formulation to date, but the ones that do exist show a reduction in inflammatory markers such as interleukin-17. Along with the reduction in inflammatory markers, human studies have also displayed improvements in dry eye symptoms, corneal staining and TBUT.25-28 Refresh Optive Mega-3 (Allergan) is a readily available and preservative-free ocular lubricant that uses flaxseed oil in its formulation; this may offer amplified clinical value over other lubricants on the market.28 Topical O3FAs have great potential and can be used in conjunction with oral O3FA supplements. However, further human studies are necessary to fully evaluate the efficacy of topical O3FAs for dry eye.
In addition to its potential mediation of dry eye, oral O3FA supplementation has demonstrated a capacity to lower the risk for other medical conditions, including atrial fibrillation, chronic kidney disease, dementia, stroke, breast cancer and retinal diseases.29-34 An eyecare professional’s responsibility extends beyond mere ocular health—O3FAs could be recommended for use in patients beyond those solely afflicted with dry eye, given their potential for enhancing overall health and mitigating risks associated with various systemic conditions.
Takeaways
The management of dry eye is far from clear cut; however, O3FAs present as one promising avenue for effective intervention. With an understanding of the intricate balance between omega-6 and omega-3 EFAs and their respective roles in inflammation modulation, clinicians can recommend nutritional supplementation to assist patients with their dry eye discomfort. Despite recent research like the DREAM study questioning the efficacy of O3FAs, the broader spectrum of evidence overwhelmingly supports their therapeutic benefits. From improving tear film stability to reducing inflammatory markers, O3FA supplementation offers a more holistic approach in managing dry eye. As eyecare professionals, it is incumbent upon us to integrate this knowledge into our practice, not only for treating this condition but also for promoting overall wellbeing. By embracing these insights, we can enhance the quality of life for countless patients troubled by dry eyes.
Dr. Shah graduated from the Illinois College of Optometry before practicing full-scope optometry in the Chicagoland area. He later joined the Center for Sight and Dry Eye Institute in Carmel, Indiana, as the Ocular Disease Resident. His primary focus is in perioperative care, glaucoma and ocular surface disease. He has no financial disclosures.
1. Takahata K, Monobe K, Tada M, Weber PC. The benefits and risks of n-3 polyunsaturated fatty acids. Biosci Biotechnol Biochem. 1998;62(11):2079-85. 2. Sadovsky R, Collins N, Tighe AP, et al. Dispelling the myths about omega-3 fatty acids. Postgrad Med. 2008;120(2):92-100. 3. Simopoulos AP. The importance of the ratio of omega-6/omega-3 essential fatty acids. Biomed Pharmacother. 2002;56(8):365-79. 4. Simopoulos AP. The importance of the omega-6/omega-3 fatty acid ratio in cardiovascular disease and other chronic diseases. Exp Biol Med (Maywood). 2008;233(6):674-88. 5. Omega-3 fatty acids fact sheet for consumers. National Institutes of Health. ods.od.nih.gov/pdf/factsheets/Omega3FattyAcids-Consumer.pdf. Updated July 18, 2022. Accessed March 14, 2024. 6. Harris WS. Fish oil supplementation: evidence for health benefits. Cleve Clin J Med. 2004;71(3):208-10,212,215-8 passim. 7. Jenkins DJA, Josse AR. Fish oil and omega-3 fatty acids. CMAJ. 2008;178(2):150. 8. Lewin GA, Schachter HM, Yuen D, et al. Effects of omega-3 fatty acids on child and maternal health. Evid Rep Technol Assess (Summ). 2005;(118):1-11. 9. Krupa K, Fritz K, Parmar M. Omega-3 fatty acids. In: StatPearls. Treasure Island (FL): StatPearls Publishing. www.ncbi.nlm.nih.gov/books/NBK564314. Updated January 17, 2023. Accessed March 14, 2024. 10. Paik B, Tong L. Topical omega-3 fatty acids eyedrops in the treatment of dry eye and ocular surface disease: a systematic review. Int J Mol Sci. 2022;23(21):13156. 11. Endres S, Ghorbani R, Kelley VE, et al. The effect of dietary supplementation with n-3 polyunsaturated fatty acids on the synthesis of interleukin-1 and tumor necrosis factor by mononuclear cells. N Engl J Med. 1989;320(5):265-71. 12. Calder PC. Polyunsaturated fatty acids, inflammation, and immunity. Lipids. 2001;36(9):1007-24. 13. Macsai MS. The role of omega-3 dietary supplementation in blepharitis and meibomian gland dysfunction (an AOS thesis). Trans Am Ophthalmol Soc. 2008;106:336-56. 14. Sullivan BD, Cermak JM, Sullivan RM, et al. Correlations between nutrient intake and the polar lipid profiles of meibomian gland secretions in women with Sjögren's syndrome. Adv Exp Med Biol. 2002;506(Pt A):441-7. 15. Hussain M, Shtein RM, Pistilli M, et al; DREAM Study Research Group. The Dry Eye Assessment and Management (DREAM) extension study—a randomized clinical trial of withdrawal of supplementation with omega-3 fatty acid in patients with dry eye disease. Ocul Surf. 2020;18(1):47-55. 16. Bermudez B, Lopez S, Ortega A, et al. Oleic acid in olive oil: from a metabolic framework toward a clinical perspective. Curr Pharm Des. 2011;17(8):831-43. 17. Miljanović B, Trivedi KA, Dana MR, et al. Relation between dietary n-3 and n-6 fatty acids and clinically diagnosed dry eye syndrome in women. Am J Clin Nutr. 2005;82(4):887-93. 18. Epitropoulos AT, Donnenfeld ED, Shah ZA, et al. Effect of oral re-esterified omega-3 nutritional supplementation on dry eyes. Cornea. 2016;35(9):1185-91. 19. Bhargava R, Pandey K, Ranjan S, Mehta B, Malik A. Omega-3 fatty acids supplements for dry eye—are they effective or ineffective? Indian J Ophthalmol. 2023;71(4):1619-25. 20. Christen WG, Cook NR, Manson JE, et al; VITAL Research Group. Efficacy of marine ω-3 fatty acid supplementation vs placebo in reducing incidence of dry eye disease in healthy US adults: a randomized clinical trial. JAMA Ophthalmol. 2022;140(7):707-14. 21. Skulas-Ray AC, Wilson PWF, Harris WS, et al; American Heart Association Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; and Council on Clinical Cardiology. Omega-3 fatty acids for the management of hypertriglyceridemia: a science advisory from the American Heart Association. Circulation. 2019;140(12):e673-91. 22. Brinton EA, Mason RP. Prescription omega-3 fatty acid products containing highly purified eicosapentaenoic acid (EPA). Lipids Health Dis. 2017;16(1):23. 23. Fabian CJ, Kimler BF, Hursting SD. Omega-3 fatty acids for breast cancer prevention and survivorship. Breast Cancer Res. 2015;17(1):62. 24. Downie LE, Ng SM, Lindsley KB, Akpek EK. Omega-3 and omega-6 polyunsaturated fatty acids for dry eye disease. Cochrane Database Syst Rev. 2019;12(12):CD011016. 25. Jacobi C, Angstmann-Mehr S, Lange A, Kaercher T. A water-free omega-3 fatty acid eye drop formulation for the treatment of evaporative dry eye disease: a prospective, multicenter noninterventional study. J Ocul Pharmacol Ther. 2022;38(5):348-53. 26. Yilmaz FO, Yildiz BK, Tunc U, et al. Comparison of topical omega-3 fatty acids with topical sodium hyaluronate after corneal crosslinking: short term results. Ocul Immunol Inflamm. 2022;30(4):959-65. 27. Cagini C, Messina M, Torroni G, et al. Efficacy of topical microemulsion of fatty acids of the ω-3 series on the sub-epithelial corneal nerves regeneration after epithelium-off corneal collagen cross-linking for keratoconus. Int Ophthalmol. 2020;40(1):205-12. 28. Downie LE, Hom MM, Berdy GJ, et al. An artificial tear containing flaxseed oil for treating dry eye disease: a randomized controlled trial. Ocul Surf. 2020;18:148-57. 29. Qian F, Tintle N, Jensen PN, et al; Fatty Acids and Outcomes Research Consortium (FORCE). Omega-3 fatty acid biomarkers and incident atrial fibrillation. J Am Coll Cardiol. 2023;82(4):336-49. 30. Ong KL, Marklund M, Huang L, et al. Association of omega-3 polyunsaturated fatty acids with incident chronic kidney disease: pooled analysis of 19 cohorts. BMJ. 2023;380:e072909. 31. O’Keefe JH, Tintle NL, Harris WS, et al. Omega-3 blood levels and stroke risk: a pooled and harmonized analysis of 183,291 participants from 29 prospective studies. Stroke. 2024;55(1):50-8. 32. Sala-Vila A, Tintle N, Westra J, Harris WS. Plasma omega-3 fatty acids and risk for incident dementia in the UK Biobank Study: a closer look. Nutrients. 2023;15(23):4896. 33. Weir NL, Guan W, Karger AB, et al. Omega-3 fatty acids are associated with decreased presence and severity of diabetic retinopathy: a combined analysis of MESA and GOLDR cohorts. Retina. 2023;43(6):984-91. 34. Zhang ZL, Ho SC, Shi DD, et al. Erythrocyte membrane n-3 PUFA are inversely associated with breast cancer risk among Chinese women. Br J Nutr. 2024;131(1):103-12. |
