Practical Matters in Myopia Management - 3rd EditionWith an expanding arsenal of information, myopia can be a puzzling area of care. In this third annual Review of Optometry supplement, experts offer solutions backed by science to help you manage this growing patient population. Click here to download a PDF or here to read the digital edition. Check out the other articles featured in this supplement: |
Myopia management is one of the fastest growing specialties in optometry that helps safeguard the ocular health of children. It provides a fun challenge and a change of pace from the typical routine exams. It is also financially rewarding as it helps decrease dependency on vision plans, which can be great for your profitability. Finally, now that the myopia epidemic has gotten more coverage in the news and myopia management has become recognized as the standard of care by the World Council of Optometry, there is an increased demand by our patients and their parents for this service.1 Maybe you do not currently provide myopia management but are thinking about adding this specialty to your clinic. Or maybe you currently provide some level of myopia management but want to take your game to the next level. Here, I’ll cover the essential items you need to do in order to provide this service to your patients.
Equipment Needed
Adding any specialty typically requires some investment up front, but fortunately the initial cost may be less than what you would expect. The most essential piece of equipment will be a corneal topographer, if you don’t already have one. If you plan to make orthokeratology (ortho-K) part of your myopia control protocol, you will need this in order to assess the cornea and troubleshoot your treatment appropriately. Topography continues to evolve, and there are some great options for this technology. However, you do not necessarily have to shell out for the most expensive topographer to be successful.
When I started, I purchased a used topographer that was pretty limited by today’s standards. It could perform topography and provide all the essential maps, but it used a very old operating system that would not allow advanced analysis of the images and was not capable of topography-based ortho-K design. It served me well until I felt ready to upgrade two to three years later. The newer topographers are more accurate, easier to use and have advanced software that allow more detailed analysis of the images. These topographers give you the capability of topography-based designs that enable you to take on more complex cases. As you get more serious about ortho-K, you will want to invest in a good topographer.
The second important expense is an instrument to measure axial length, which is vital for both assessing risk in patients as well as tracking the effectiveness of your treatment. The least expensive option would be an A-scan; however, optical biometry is much more convenient for both your staff and the patient, as it is non-contact and does not require the use of topical anesthetics. Given that your target patients are children, this can be an important consideration. In addition, the A-scan is much more reliant on user technique and is less reliable and repeatable than an optical biometer. Many of the newer biometers on the market include software that allows you to plot the patient’s axial length on a growth curve, which is very helpful for patient/parent education and also for measuring your success.
 |
|
The Cary Family Eye Care Myopia Control team (left to right): Kristen McGarvey (Myopia Control Coordinator), Dr. Dwight Barnes, Dr. Rachel Kormos and Bryce Poole (Clinic Assistant). Click image to enlarge. |
If biometry is not immediately within your budget, don’t let that stop you from getting started! While this information is very important, you could add biometry later on after you’ve gotten started. The decision of when to add a biometer will likely depend on the volume of myopia management that you are doing, as it is easier to justify the cost if you are using it frequently. However, biometry can also be a powerful tool to grow your myopia practice. By measuring axial length on all young patients, you can identify at-risk patients and better illustrate to parents the need for myopia management. Keep in mind that as biometry has become more common, there are devices available that combine biometry with other measurements such as topography or auto-refraction. This can be helpful especially if space is limited in your office.
Acquiring Knowledge
With the recent growth of myopia management, there is an abundance of options for learning how to provide this service. One of your best resources for learning about ortho-K will be the lab consultants. They know their designs extremely well and can assist with troubleshooting while also explaining the “why” behind the changes needed. Many of these lens designs have a certification process that can teach you all the basics of that design. While all ortho-K designs use the same basic principles, they often use different terminology to describe various aspects of the lens. It is important to learn the basics of ortho-K as well as the nuances of the specific design you plan to use. This can ensure accurate communication with the consultants for the lab. Be sure to learn about all available treatment options so you can provide the best treatment for each individual patient. Besides ortho-K, the other current treatment options here in the United States are dual-focus soft contact lenses and atropine.
A great option for rapidly achieving a high level of knowledge about myopia control are large conferences like the Vision by Design meeting by the American Academy of Orthokeratology and Myopia Control (AAOMC; aaomc.org) and the Global Specialty Lens Symposium (GSLS) by Contact Lens Spectrum. Live, in-person events like these offer the added benefits of condensing a lot of education into one weekend. They also generate excitement about this specialty by networking with other like-minded clinicians. Vision by Design includes a Boot Camp program specifically for those clinicians who are new to this specialty. Other options for training include optometry journals, online continuing education and websites such as myopiaprofile.com, reviewofmm.com and bhvi.org. Sometimes the best information can come from a more experienced colleague. If you know of another optometrist who is successfully providing myopia management services, reach out to them with your questions. Early on in my quest to learn more about myopia management, I benefited tremendously from the knowledge of other optometrists who were willing to serve as a mentor.
 |
| Click image to enlarge. |
Setting Your Fees
Doing this appropriately is important to ensure you are profitable with myopia management. These patients typically require multiple visits per year. Given the potential investment in equipment, the additional time spent with the patients and the cost of materials, it is essential to set your fees appropriately to ensure you are adequately compensated for your efforts. While there is not a specific formula that will apply to all practices, I advise to start by learning your chair cost. This is the cost of running your clinic per hour. If you know your chair costs, the cost of the materials (e.g., ortho-K lenses, soft dual focus lenses) and the number of visits expected per patient, you can begin to calculate appropriate fees. Don’t forget to factor in potential ortho-K design changes requiring additional lenses to be ordered and the profit you want to generate after paying for your clinic costs and materials. This specialty has tremendous benefits to the patient, so don’t be afraid to charge what you are worth.
Other Items at the Start
One of the other tasks needed is to create an informed consent document. This document provides information about the proposed treatment, explains how the treatment works, what is involved for the patient, expectations, risks and benefits. It helps to ensure that the patient and the parent fully understand what to expect and allows them to acknowledge they have been fully educated as to the specifics of treatment. You can have a separate informed consent for each treatment modality, or you can have one document that includes all treatments. Other items to consider including in your informed consent would be information related to FDA approval. While the treatments we provide are FDA approved for safety, in many cases, the FDA approval is not specifically for myopia management (one notable exception is CooperVision’s MiSight lens, whose FDA approval is specific for slowing myopia progression).2 I find it’s also helpful to have documentation for the parents to sign acknowledging the costs involved with treatment and any refund policy so there are no surprises. This can be included in the informed consent or can be a separate document.
 |
|
A technician captures a topography image. High-quality topography images are essential for tracking ortho-K outcomes. Click image to enlarge. |
In order to use atropine as a treatment option, you will need to establish a relationship with a local compounding pharmacy or find an online compounding pharmacy that will ship to your patients. A compounding pharmacy is needed since myopia management uses lower concentrations of atropine than what is commercially available. Not all compounding pharmacies are willing to make ophthalmic preparations, so be sure to confirm that they are able to provide the most common atropine concentrations that you plan to use. Let patients know what potential side effects to expect from atropine. The most common side effects are near blur and photophobia. The benefits of atropine are dose-dependent, and so are the side effects.
If patients are bothered by side effects, they can often be managed by using glasses with photochromic lenses and/or bifocal lenses. However, for most patients, atropine is well-tolerated. In our clinic, we prescribe photochromic lenses for all atropine patients, and also lenses with a near “boost” technology. We rarely find that we need to prescribe a true bifocal lens.
If you plan to fit ortho-K, determine which design to use. There are many options for ortho-K designs, so if you are not sure where to start, speak to representatives and consultants to gather more information to make your decision.
There are three different ways for a practitioner to design and order these lenses: trial lens fitting, ordering empirically and custom design using software. For trial lens fitting, a doctor uses a set of diagnostic lenses to evaluate the fit on the eye, and then either dispenses from the kit or orders the needed lens from the lab. For empirical design, the clinician provides key data such as the refraction, keratometry and corneal diameter to the lab, so that the lab consultants can create the design. For software design, the clinician creates a very customized design using software and sends the design to the lab for fabrication.
For the novice fitter, designing the lens using trial lens fitting or ordering empirically will be easier. However, over time, many doctors move to designing their own lenses using software, as it gives you a tremendous amount of control over the final product. Go through the certification process for any ortho-K, soft dual focus or extended-depth of-focus (EDOF) lens options you plan to use and learn the process of ordering from the labs. The certification process is often quick, sometimes taking no more than a couple of hours. Request diagnostic fitting sets for soft lenses that you plan to use as well as ortho-K, if needed.
 |
|
A technician obtains axial length measurement. Optical biometry is the best way to track myopia progression. Click image to enlarge. |
Getting Your Staff on Board
Even if you are a myopia control expert, you must have your team on board in order to effectively communicate with patients so they are aware that you provide this service. Many parents do their own research prior to calling to schedule, so you want your team to be prepared to provide accurate information. One of the most helpful strategies we used was to create a large FAQ document for our team. This allows them a resource to feel confident answering the most common questions. You and your team can slowly add to this document as new questions are encountered.
Examples of common FAQs are “How many nights do I need to wear the ortho-K lenses to fully correct my vision?”, “Will the lenses hurt?”, “What makes dual focus myopia control soft lenses different from regular soft lenses?”, “How do they work to slow myopia progression?” and “Is it OK if I miss a night of wear?”
Some of your vendor partners will also be able to provide training. For example, in addition to a MiSight certification program for clinicians, CooperVision provides additional training resources for staff. You can use some of your staff training time to present to your team and teach them about myopia control.
Be sure to explain to your staff how it benefits both your patients and your practice. Get your staff excited about this service, and they will promote it to your patients. Offer ortho-K to your staff members so they can experience the benefits firsthand. If any of your team members have myopic children, provide myopia management for them.
As you get busier with providing myopia services, it is helpful to appoint a myopia control coordinator on your staff. This person can be responsible for following up with interested parents, scheduling myopia control consults, training patients on handling contact lenses, tracking and receiving orders for patients, ordering myopia management supplies and helping to educate the rest of your team. Your myopia control coordinator can also be responsible for discussing fees with patients and going through the initial enrollment paperwork. It’s helpful to have a trusted team member to cover the fees so the doctor can focus on the evaluation and treatment recommendations.
If you are interested in appointing a myopia control coordinator, consider enrolling a team member in the Certified Myopia Navigator (CMN) accreditation program through the AAOMC. This program helps your staff members develop a higher level of expertise to really drive your myopia clinic forward.
 |
|
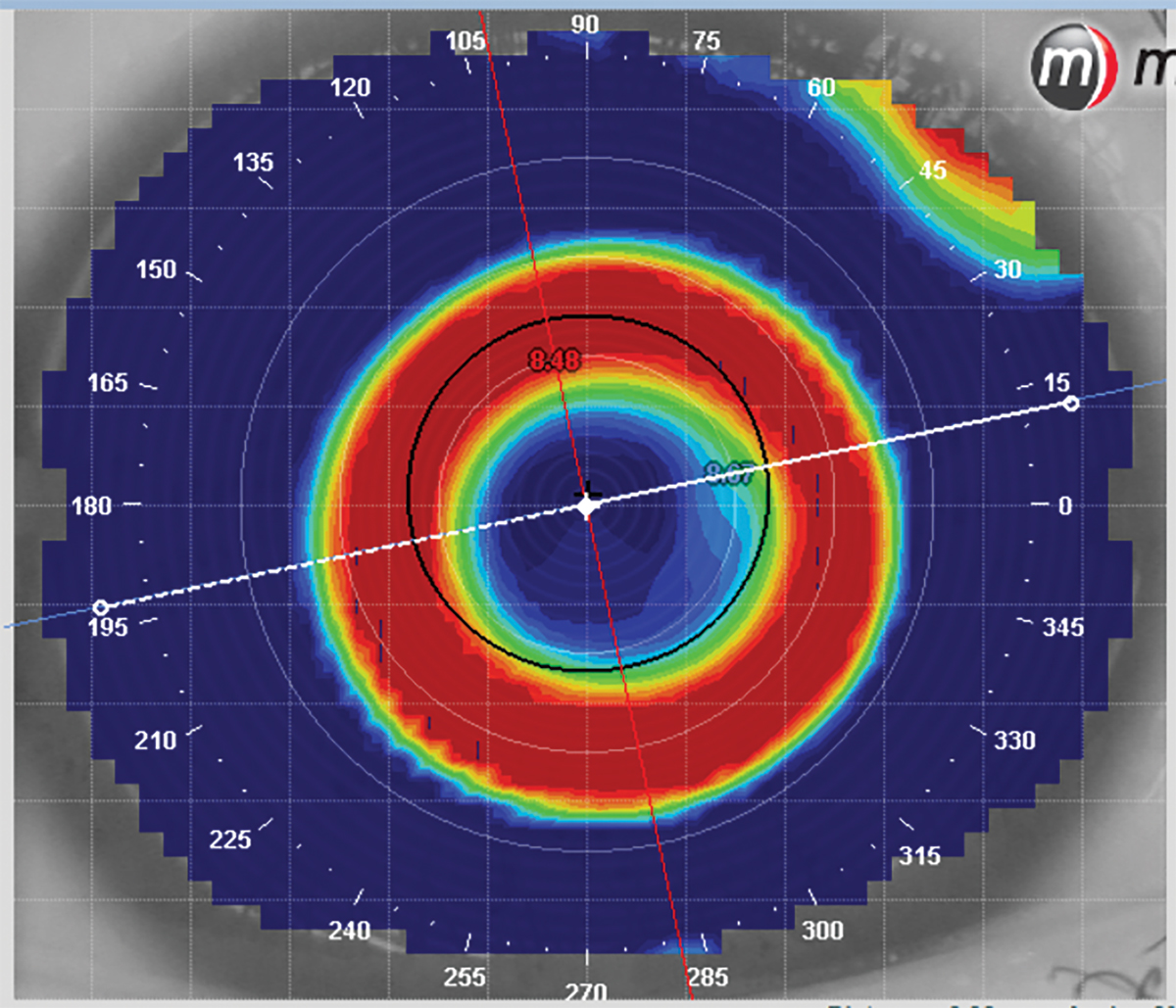
Post-treatment ortho-K image. Analyzing the post-treatment topography is important to assess how the lens is performing. Click image to enlarge. |
Presenting to Your Patients
Once you have purchased any necessary equipment and learned how to provide this service, it’s time to get started and present this to your patients! If you focus your marketing efforts on internal marketing as opposed to external marketing, there are several inexpensive ways to promote myopia control. You should add this service to your website with some information related to its importance. You can create brochures or handouts for your patients to help reinforce the information you present during the examination. If you don’t want to create your own customized brochures, there are ready-made options from vendor partners and from the AAOMC. Consider signage in your office to help generate awareness.
One of my goals in creating my internal marketing was to make it nearly impossible for a patient to make it all the way through an exam at our office without becoming aware that we offer this service and that we are experts at it. Remember, even if the patient in your chair is not a candidate for myopia control they may have a family member or other acquaintance who would benefit from it.
When seeing parents in the chair, ask them about their children and if they’ve had an eye exam recently. Finally, keep in mind that it is your duty as the doctor to present this option to all potential patients. Children who are nearsighted get more so as they age, so when you see a young myope it is your duty of care to educate the parents.
Let parents know that myopia gets worse over time, that higher myopia increases the risk of vision loss and that you can help with that. If you have the ability to measure axial length, it can be beneficial to plot that on a growth chart for the parents. Since parents are already familiar with height and weight growth curves from the pediatrician, they can quickly understand the information when presented in this manner. Armed with this information, most parents will be very interested in doing something to slow down the progression. Once you’ve provided this information, you can have your team schedule the patient for a myopia control consultation with you.
Scheduling a Consult
It is worth mentioning that not every doctor schedules patients for a separate consult visit. It is possible to initiate treatment immediately at the comprehensive exam. However, given the greater number of questions many parents have about this service, I find it is very helpful to schedule a consultation visit. Some doctors charge a fee for this, and others do not. If charging a fee for the consultation, you may choose to credit that fee toward the treatment program if the patient moves forward with treatment. When consulting with a family, remember to engage the patient directly instead of only talking to the parents. This allows you to build a relationship with your young patient that will increase their trust in you.
 |
|
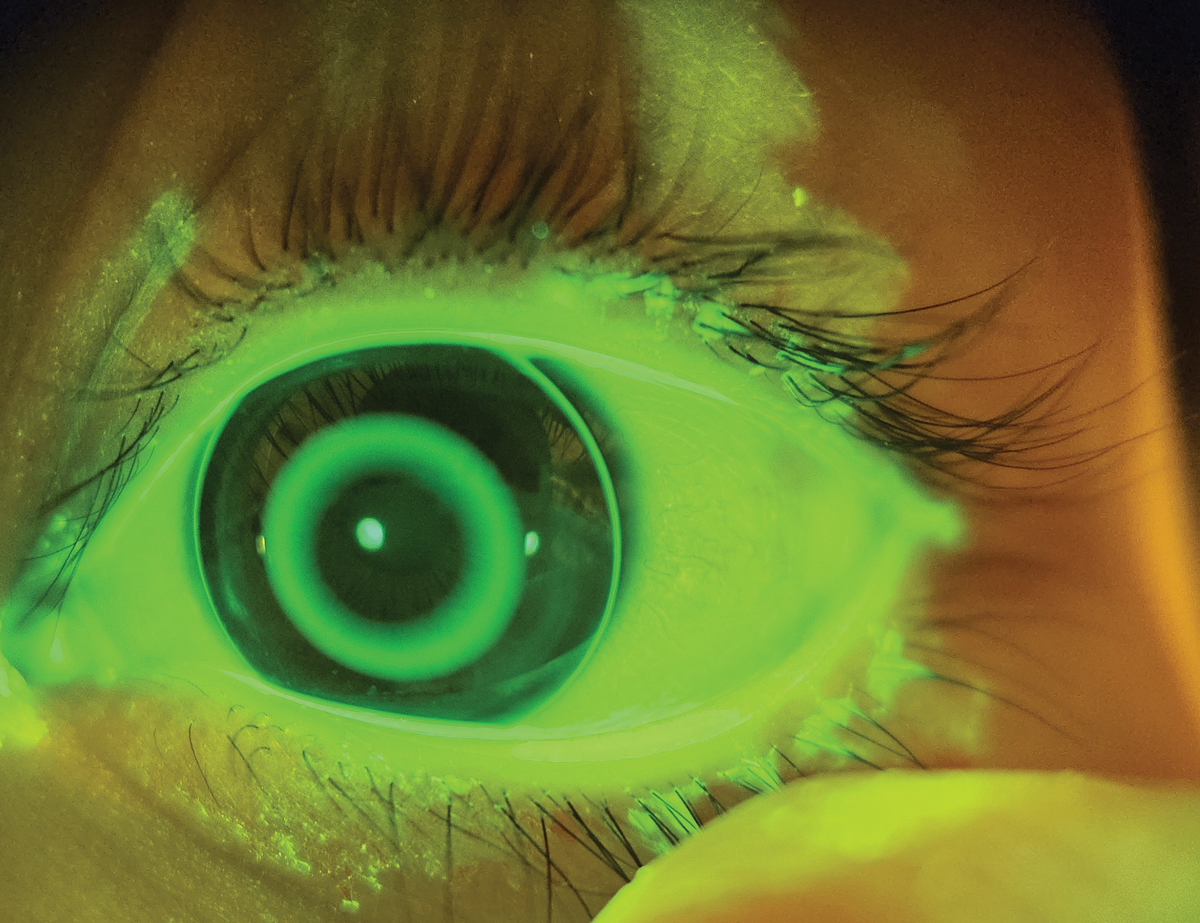
A fluorescein image of an ortho-K lens. Fluorescein is used to help assess the lens fit. If needed, NaFl images can be sent to a consultant for assistance with troubleshooting the fit. Click image to enlarge. |
When speaking to a young patient, it’s important to develop a rapport to make them feel comfortable. Try to identify and address any potential concerns they may have. The most common questions in my experience are related to whether the treatment will hurt. This could apply to contact lenses or an eye drop. In order to reduce apprehension, when fitting a contact lens I will talk the patient through the process, explaining as I go along. This helps the patient feel more comfortable.
If you plan to recommend ortho-K, you can evaluate diagnostic lenses at the myopia consultation. This is not absolutely necessary if you plan to order lenses empirically or use a software to design the lenses. However, it can still be very helpful to assess the patient and give them an idea of what the process is like. The amount of time needed will depend on your staffing levels and how much you choose to delegate. After gathering all required information and evaluating the refraction, topography, axial length, prior history of progression, parental history of myopia and other pertinent data, make a treatment recommendation and present that to the parents and child.
Additional Tips for Success
Once you’ve completed your checklist for implementation, go ahead and pick out a suitable candidate and get started! There is no substitute for experience, and the best way to gain experience is to actually see patients. Especially with ortho-K, there is a learning curve to get comfortable. It can be helpful to start as easy as possible by looking for the “low hanging fruit”. Keep an eye out for low to moderate myopic patients without much astigmatism. Higher levels of myopia and moderate astigmatism increases the difficulty of achieving a great outcome. Over time, you’ll likely get comfortable tackling more challenging cases, but starting off with more straightforward cases helps you to get comfortable with what you’ve learned and your newly acquired tools. The learning curve for myopia control soft lenses is much quicker.
Once you understand the how and why the soft lenses work, the actual fitting process is quite easy and is similar to other soft disposable lenses. I love myopia management because it allows me to see primarily children (who are more fun to interact with than adults), allows me to help people and it’s a fun challenge. As with other specialty care, myopia management is continually evolving so there is always more to learn. New products and technology are coming out every year, so continuing education is essential. Invest the time into learning about these new products and gaining more expertise. As a result, you will provide the most effective treatment for your patients.
Dr. Barnes is co-founder of Cary Family Eye Care in Cary, NC, and he is clinical director of its Myopia Control Clinic. He is a fellow of the American Academy of Orthokeratology and Myopia Control (AAOMC) and serves on the AAOMC board of directors. He also holds the designation of International Academy Certification in Myopia Management (IACMM). He has been paid as a speaker and consultant by CooperVision, Vyluma and Barti.
1. Standard of care guidelines for myopia management. World Council of Myopia. myopia.worldcouncilofoptometry.info/standard-of-care. Accessed July 1, 2024. 2. Chamberlain P, Bradley A, Arumugam B, et al. Long-term effect of dual-focus contact lenses on myopia progression in children: a six-year multicenter clinical trial. Optom Vis Sci. 2022;99(3):204-12. |
