 |
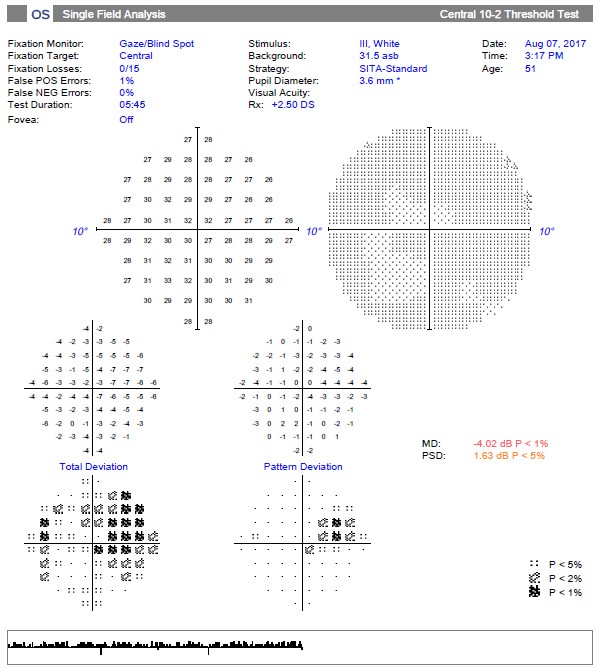
Study shows 10-2 VF testing doesn’t detect any additional defect not already seen on 24-2 testing, but it provides sufficient additional information for patients with a repeatable defect within the central 12 locations of the 24-2 VF test. Photo: Danica Marrelli, OD. Click image to enlarge. |
In a new Ophthalmic Technology Assessment by the American Academy of Ophthalmology, researchers evaluated the current published literature on the utility of the 10-2 visual field (VF) testing strategy for the evaluation and management of early glaucoma, defined here as mean deviation (MD) better than -6 decibels (dB). They concluded that 10-2 VF testing may not be the most useful routine test for patients with early glaucoma, but would provide sufficient additional information for patients with a repeatable defect on the pupillary distance (PD) plot among the central 12 points on the 24-2 or 24-2C VF test. Their results were recently published in the Ophthalmology journal.
After review, 26 articles in the PubMed database were selected; the panel methodologist rated them for strength of evidence. Thirteen articles were rated level I and eight articles were rated level II, while five level III articles were excluded. Data from the 21 included articles were abstracted and reviewed.
Results from the study found that the central 12 locations on the 24-2 VF test grid lie within the central 10° covered by the 10-2 VF test. In early glaucoma, defects detected within the central 10° generally agree between the two tests. Defects within the central 10 degrees of the 24-2 VF test can predict defects on the 10-2 VF test, although the 24-2 may miss defects detected on the 10-2 VF test.
“In addition, results from the 10-2 VF test show better association with findings from OCT scans of the macular ganglion cell complex,” the authors noted in their report. “Modifications of the 24-2 test that include extra test locations within the central 10 degrees improve detection of central defects found on 10-2 VF testing.”
The authors explained that central VF defects may be underappreciated in the evaluation of early glaucoma. “Although less common in cases in which MD is better than e6 dB, central defects may have a profound impact on a person’s visual function and quality of life. Thus, detection of central VF defects is essential in the diagnosis and management of glaucoma even at the earliest stages,” they explained.
With the extra central test locations, the Zeiss 24-2C or the Octopus G1 test strategies can improve detection of central defects over the standard 24-2 VF, the authors added. Although the 10-2 VF is considered the gold standard for detecting central VF defects, it’s more involved for both the patient and clinician, as it entails additional time, cost and effort, and it may not always detect any additional defect not already seen on 24-2 testing.
“Thus, the evidence to date does not support routine testing using 10-2 VF for patients with early glaucoma,” the authors concluded. “Recent studies (level I and II) provide some evidence on additional VF testing in some cases, however. Early 10-2 VF testing would provide sufficient additional information for any patient with a repeatable defect on the PD plot among the central 12 points on the 24-2 or 24-2C VF test or with a depressed average and/or minimum mGCIPL thickness on SD-OCT. A defect detected on SAP 10-2 VF warrants confirmation and potentially a lifelong commitment to serial 10-2 VF testing.”
WuDunn D, Takusagawa HL, Rosdahl JA, et al. Central visual field testing in early glaucoma. Ophthalmology. December 8, 2023. [Epub ahead of print.] |
