 |
A 68-year-old African American male presented to the clinic for a routine eye examination with a chief complaint of blurred vision OS of many months’ duration. His ocular history was remarkable for cataracts and blunt trauma OU. His systemic history was remarkable for appropriately treated hypertension and diabetes. He denied allergies to medications. His best-corrected entering visual acuities were 20/20 OD and 20/30 OS at distance and near, with no improvement upon pinhole or refraction. His external examination was normal with the exception of the facial Amsler grid OS. There was no afferent defect.
Biomicroscopic exam demonstrated normal anterior segment tissues with grade II nuclear sclerotic cataracts, present in both eyes. His intraocular pressures measured 16mm Hg by Goldmann applanation tonometry. The pertinent posterior segment findings are demonstrated in the photographs and OCT scans shown here.
 |
|
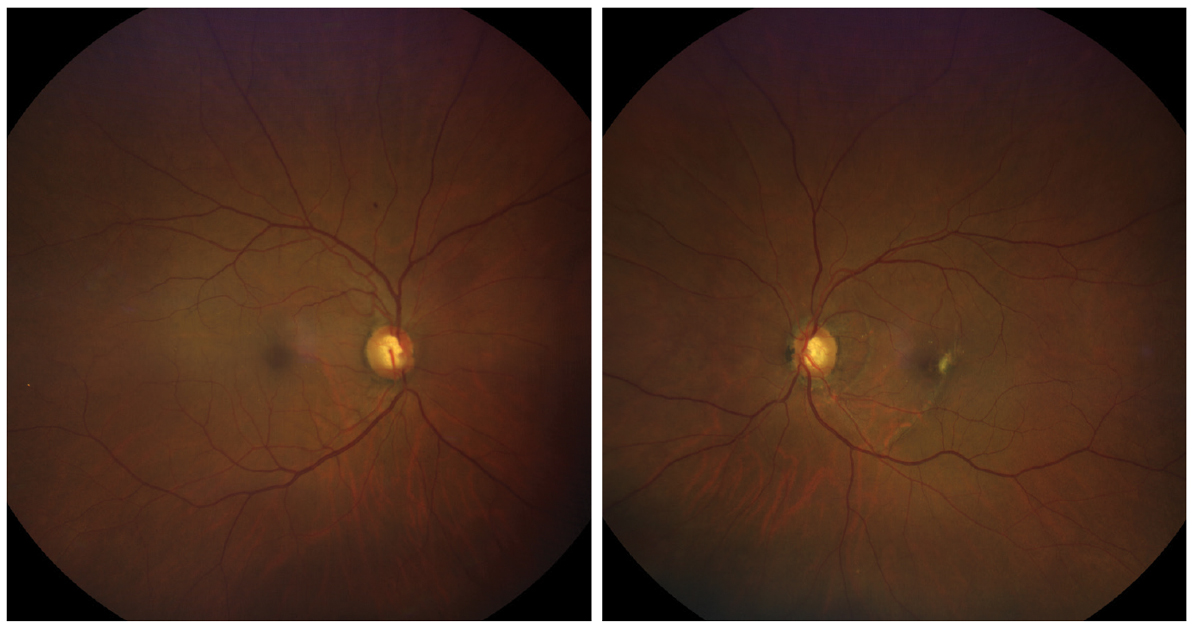
Fundus examination revealed the following presentations. Does this match the case history? Click image to enlarge. |
Additional Testing
A traditional Amsler grid revealed some relative scotomata and metamorphopsia centrally OS; this was substantiated upon formal automated perimetry. Additional funduscopic examination was completed with a 90-diopter lens; there was no Watske-Allen sign (vertical strip of light perceived by the patient as “broken” or distorted). OCT testing was completed, uncovering the clear diagnosis. A laser interferometer could also have been used to assess best acuity under the current conditions, showing little improvement. Color photography was also completed for the purposes of documentation.
Diagnosis
The principal finding in this issue is choroidal rupture (CR) from a previous motor vehicle accident. The secondary finding was “talc-retinopathy” OU.
CR is a possible consequence of blunt trauma to the eye or its adnexa.1-7 Patients developing choroidal rupture are often younger males involved in activities such as ball sports, which exposes them to high-speed impact. While it seems that men are more likely to experience blunt ocular trauma, one report indicated that choroidal rupture occurred more often in women.7 Common causes of choroidal rupture include impact injuries from paintballs, bottle corks, elastic bands, airbags and sports equipment, among numerous others.8-12
Choroidal ruptures may be single or multiple and may affect any part of the posterior segment.2,13,14 They are not typically seen acutely secondary to acute hemorrhages, which may occur in any layer of the eye ranging from the choroid to the vitreous after the traumatic injury.3,15 In cases of old CR caused by trauma many years prior, you may see subretinal, intraretinal or preretinal scarring or hemorrhage if choroidal neovascularization formed and bled.16,17
The patient’s visual acuity and visual field may be unaffected depending upon the location of the choroidal rupture and degree of collateral damage produced by the trauma. Unfortunately, the detection of a choroidal rupture often signals the risk for significant damage throughout the eye.7 Patients may have variably reduced acuity if the rupture occurred within the posterior pole. Acuity may be drastically affected in cases that have subfoveal involvement.10-12,14,15
Ophthalmoscopically, there is a posteriorly located curvelinear (crescent-shaped) disruption parallel to the ora serrata. Often, the rupture will have a concave aspect angled toward the disc. Many ruptures are concentric with the optic nerve. They are frequently vertically oriented consistent with breaks in Bruch’s membrane.2 There is usually significant active retinal pigment epithelium (RPE) hyperplasia, giving the rupture a pigmented appearance. The sclera can be variably seen beneath the lesion depending upon the degree of damage and exposure of the underlying tissue.
Direct or indirect injury can precipitate choroidal rupture. Direct ruptures are usually located anteriorly, at the exposed part of the eye and parallel to the ora serrata.18 More common are indirect ruptures occurring in the posterior pole. These are the classic, concentrically appearing defects.18 As the globe is compressed along an anterior-posterior vector, the globe expands laterally, often resulting in a break in Bruch’s membrane. In most cases, the sclera maintains the globe’s integrity, limiting the damage to the resultant choroidal rupture along with any collateral injuries sustained as a result of the trauma. Unfortunately, in some cases the sclera tears, producing a ruptured globe.4,6,7
In CR, hemorrhages and edema presenting initially will resolve. Typically, retinal and choroidal pigment epithelial hyperplasia gives the rupture a heavily pigmented appearance. Often, the overlying retina is undisturbed. However, in the event the RPE is damaged it may become hyperplasic, invading the neurosensory retina, producing visual dysfunction.
Two distinct tomographic patterns of choroidal ruptures have been identified. The first type involves a forward protrusion of the RPE-choriocapillaris (RPE-CC) layer; here, an acutely angled pyramid or dome shape forms. This is associated with either a small loss of continuity of the RPE layer or elevated RPE-CC projection accompanied by a significant quantity of subretinal hemorrhage. The second type choroidal rupture pattern involves a larger area of disruption of the RPE-CC layer; here, the photoreceptor inner segment/outer segment junction and external limiting membrane are involved, with a posterior-directed concave contour depression in the area with downward sliding of tissues into the defect.19
The subsequent disruption of Bruch’s membrane in choroidal rupture creates the possibility for the development of choroidal neovascular membranes.13,14,16,17-20 This may be a late development, which often occurs years after the precipitating trauma.18,21 Several factors have been seen to be predictive of choroidal neovascular membranes in choroidal rupture; namely, proximity of the rupture to the center of the fovea, longer length of the rupture, older age at the time of the injury and macular choroidal rupture.13,14 Patients with these factors should be monitored closely.
Management Options
There is no intervention in the acute phase of choroidal rupture, as long as the sclera is intact with no rupture of the globe. The acute management is directed toward the treatment of traumatic uveitis, hyphema, retinal detachment or breaks and issues pertaining to elevated intraocular pressure. Patients with choroidal ruptures should be educated about their condition and counseled to consider full-time safety eyewear (protective frame with polycarbonate lenses). The patient must be monitored funduscopically for the development of choroidal neovascularization. The use of home Amsler grid monitoring is recommended.
Various therapeutic modalities have been used to treat choroidal neovascularization occurring from choroidal rupture. Thermal laser photoablation has been a mainstay for these membranes.14,18 Photodynamic therapy (PDT) has been used with success.20-22 PDT often results in reduction of membrane leakage and can completely eliminate the membrane with few adverse effects. Surgical removal of the neovascular membranes has also been reported.17 Subsequent submacular hemorrhage has been managed with vitrectomy, subretinal injection of tissue plasminogen activator and pneumatic displacement of blood with intravitreal air tamponade.23,24
It has also been reported that intravitreal injection of an anti-VEGF agent has shown impressive results in managing choroidal rupture with associated choroidal neovascularization and subretinal fluid.25-29
 |
|
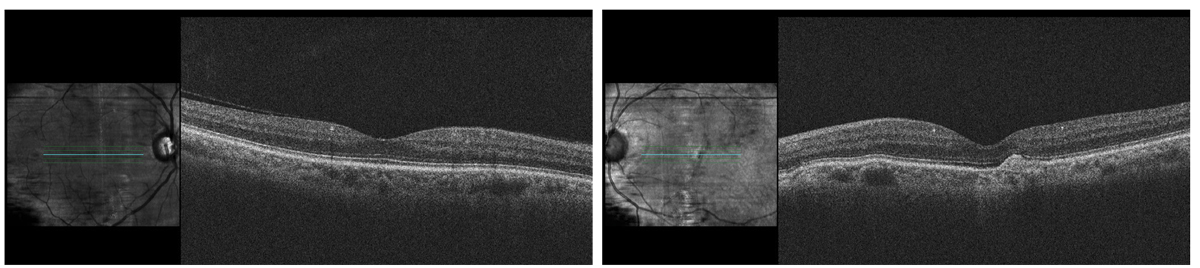
Do the OCT scans seen here give you more information about the patient’s ocular status? Which findings are most pertinent to the case? Click image to enlarge. |
Prognosis
While choroidal rupture involving the macula tends to have a poor visual prognosis, there are reported cases of patients with foveal choroidal ruptures regaining central vision over a protracted recovery period.30 There also have been reports of early progression of choroidal rupture with subsequent loss of vision.31
Patients with CR should be considered for late traumatic glaucoma; photographs of the CR should be taken and baseline testing completed. Gonioscopy should be completed after the acute injuries are resolved to observe the angle’s status. Biannual intraocular pressure measurements are recommended to insure stability.
Talc retinopathy is defined by irregularly shaped refractile yellow intraretinal deposits.32 It is a phenomenon observed in long-term intravenous drug users who crush and inject or inhale medications.32 Talc retinopathy is a risk factor for the formation of intraretinal emboli and neovascularization, typically forming in the peripheral retina.33 Most of the time, talc retinopathy poses minimal risk to the eye, however, it does imply systemic inundation of the foreign particles that created it.33 In cases that threaten the macula or visual functioning, sectoral panretinal laser photocoagulation can be performed in an attempt to regress the neovascular net.34
Take-home Points
Some notable lessons to remember from this case:
- Patients with CR typically retain excellent visual function and often present asymptomatically years after the causing trauma.
- Associated choroidal neovascularization may occur years after the CR-causing trauma has been forgotten.
- CNV resulting from choroidal rupture, like other CNV, may spontaneously involute, making close observation an option when there is no imminent threat to vision.
- Gonioscopy should be performed on all patients with CR to rule out angle damage and an increased risk for developing late traumatic glaucoma.
- Small peripheral choroidal ruptures can be confused with retinal lattice degeneration; true lattice lesions are typically located anterior to the equator while peripheral choroidal ruptures are posterior.
Dr. Gurwood thanks Megan Cruce, OD, for her contributions to this case.
Dr. Gurwood is a professor of clinical sciences at The Eye Institute of the Pennsylvania College of Optometry at Salus University. He is a co-chief of Primary Care Suite 3. He is attending medical staff in the department of ophthalmology at Albert Einstein Medical Center, Philadelphia. He has no financial interests to disclose.
