 |
In August, a Manhattan jury awarded a former investment banker a record $7.25 million in damages for vision impairment he attributed to LASIK. The plaintiff claimed that he suffered distorted and blurred vision, particularly in his left eye, eight months after the procedure because doctors failed to diagnose keratoconus.
To avoid similar lawsuits, we need a greater understanding of postoperative ectasia and its potential warning signs before we refer patients for LASIK. Here, well review some of the latest research on this potentially debilitating disorder.
Mapping Out Keratoconus
Keratoconus is a bilateral progressive disease, and although moderate or advanced cases should be detectable, mild cases often are not clinically pronounced.1 However, LASIK performed even on a mild or early form of keratoconus or forme fruste (atypical) keratoconus usually results in late-stage ectasia.2,3
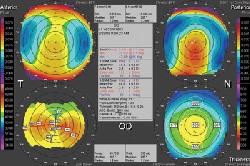 |
| This patient shows early warning signs of forme fruste keratoconus including a posterior float >50m, K values >46.00D, a variance of cylinder between eyes and three abnormal maps. |
One such indicator: the number of abnormal maps. Specifically:
One abnormal map does not usually indicate forme fruste keratoconus. Still, you should educate the patient, or have him or her return in six to 12 months to check for changes to the corneal surface.
Two abnormal maps may indicate early keratoconus. An abnormal posterior float with a slightly thinner cornea (<500m) may indicate keratoconus depending on other variables listed below. If topography does not indicate forme fruste keratoconus but there are two abnormal maps, surface ablation would likely be a better procedure than LASIK.
Three or more abnormal maps mean that corneal surgery is contraindicated. These patients have a high risk of developing ectasia.
Additional Indicators
There are several other indicators to help you gauge a patients risk of ectasia. These include:
Keratometry. Although this is still a good indicator of ectasia, you may need to measure beyond the central 3mm of the cornea because keratoconus and pellucid marginal degeneration (PMD) often affect the mid- and peripheral cornea.4
Corneal topography systems have an irregularity index that shows the variation between the highest and lowest points within 3mm, 5mm or 7mm, depending on the unit. Any irregularity >1.50D at 3mm and 2.00D at 5mm on the Orbscan or >1.40D steepness on systems that use the Rabinowitz or Klyce indices is a red flag for ectasia. One note: On the Orbscan, irregularity at 3.00mm and 5.00mm may simply reflect higher-order aberrations; use this index in conjunction with other findings to diagnose keratoconus.
Some researchers believe that all keratoconus begins on the posterior corneal surface.5 Using the posterior float, a reading >0.050mm raises a strong red flag for forme fruste keratoconus or PMD and confirms it if other maps and measurements support it.6,7 Also, when the float is >0.040mm (and in some cases as low as 0.035mm with other corresponding abnormal maps), significant inferior thinning that matches the steepest posterior apex should raise suspicion for early forme fruste keratoconus.8 A thin cornea is not necessary to confirm a high risk of ectasia.9
Corneal thickness. Research at our center suggests that a peripheral (usually inferior) cornea that is not 20m thicker than the central pachymetry raises suspicion for forme fruste keratoconus or an increased risk of post-LASIK ectasia. The peripheral cornea normally shows significant thickening from the central cornea.10
Cylinder. A difference in cylinder between the two eyes and/or increasing cylinder is an early indicator of keratoconus.9,11 One eye usually progresses faster than the other.12 A difference >1.00D between the eyes should raise your suspicion.
Higher-order aberrations. An increase in higher-order aberrations might also be an indicator of early keratoconus.13 Research indicates that early keratoconus manifests with an increase in coma, and early PMD manifests with an increase in trefoil, quadrafoil and pentafoil (>0.35m) or peripheral aberrations, as would be expected from a condition that affects the peripheral cornea.14
These indicators help identify patients at risk of post-LASIK keratectasia. If one or more indicators are suspicious, have the patient return in six-months for repeat measurement. Most patients we reviewed who developed ectasia had four or more of the indicators listed above.
An understanding of early-stage and forme fruste keratoconus is critical for preventing post-LASIK ectasia, preserving the patients visual quality and protecting your practice from lawsuits.
Dr. Karpecki, director of research at Moyes Vision Center, is a consultant to Bausch & Lomb but has no financial interest in the products mentioned.
1. Weed KH, McGhee CN. Referral patterns, treatment management and visual outcome in keratoconus. Eye 1998;12(Pt 4):663-8.
2. Buzard KA, Tuengler A, Febbraro JL. Treatment of mild to moderate keratoconus with laser in situ keratomileusis. J Cataract Refract Surg 1999 Dec;25(12):1600-9.
3. Randleman JB, Russell B, Ward MA, et al. Risk factors and prognosis for corneal ectasia after LASIK. Ophthalmology 2003 Feb;110(2):267-75.
4. Edrington TB, Szczotka LB, Begley CG, et al. Repeatability and agreement of two corneal-curvature assessments in keratoconus: keratometry and the first definite apical clearance lens (FDACL). CLEK Study Group. Collaborative Longitudinal Evaluation of Keratoconus. Cornea 1998 May;17(3):267-77.
5. Charles N, Charles M, Croxatto JO, et al. Surface and Orbscan II slit-scanning elevation topography in circumscribed posterior keratoconus. J Cataract Refract Surg 2005 Mar;31(3):636-9.
6. Arntz A, Duran JA, Pijoan JI. Subclinical keratoconus diagnosis by elevation topography. Arch Soc Esp Oftalmol 2003 Dec; 78(12):659-64.
7. Rao SN, Raviv T, Majmudar PA, Epstein RJ. Role of Orbscan II in screening keratoconus suspects before refractive corneal surgery. Ophthalmology 2002 Sep;109(9):1642-6.
8. Rao SN, Epstein RJ. Early onset ectasia following laser in situ keratomileusus: case report and literature review. J Refract Surg 2002 Mar-Apr;18(2):177-84.
9. Twa MD, Nichols JJ, Joslin CE, et al. Characteristics of corneal ectasia after LASIK for myopia. Cornea 2004 Jul;23(5):447-57.
10. Liu Z, Zhang M, Chen J et al. Corneal topography and thickness in keratoconus. Zhonghua Yan Ke Za Zhi 2002 Dec;38(12): 740-3.
11. Chopra I, Jain AK. Between eye asymmetry in keratoconus in an Indian population. Clin Exp Optom 2005 May;88(3):146-52.
12. Zadnik K, Steger-May K, Fink BA, et al. Between-eye asymmetry in keratoconus. Cornea 2002 Oct;21(7):671-9.
13. Barbero S, Marcos S, Merayo-Lloves J, Moreno-Barriuso E. Validation of the estimation of corneal aberrations from videokeratography in keratoconus. J Refract Surg 2002 May-Jun;18(3): 263-70.
14. Maeda N, Fujikado T, Kurada T, et al. Wavefront aberrations measured with Hartmann-Shack sensor in patients with keratoconus. Ophthalmology 2002 Nov;109(11):1996-2003.
