 |
||
|
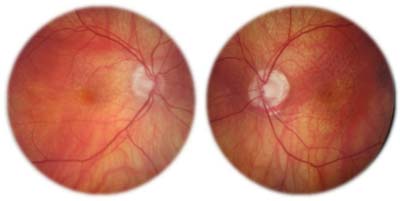
Dilated fundus examination of our 78-year-old patient. Medical history includes benign prostate enlargement with a low PSA. Should supplements be modified?
|
Would you modify his current supplement regimen?
The Benefits of Fish Oil
Inflammation is a known contributing factor in various distinct systemic and ocular conditions. Thus, the anti-inflammatory activity of omega-3 supplementation is of primary interest to both patients and health care professionals. A number of debatable health benefits are associated with increased intake of the long-chain omega-3s, eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA).1-11
• AMD. In the past, omega-3 supplementation has been shown to decrease the prevalence and progression of AMD. However, the first published results from AREDS2 indicated that fish oil supplementation had no impact on progression toward more advanced disease stages.12,13
• Heart disease. A recent study determined that there was insufficient evidence to support previous findings that omega-3 FAs reduced the risk of cardiovascular-related mortality or morbidity.14
• Prostate cancer. Several studies have shown an inverse correlation between omega-3 FAs and prostate cancer.5-12 One such study indicated an associated risk reduction for prostate cancer among men who ate fish at least three times a week.8 A separate study followed 45,000 men for 14 years and found an association between high-level EPA and DHA intake and reduced incidence of prostate cancer.11
The SELECT Study
The original Selenium and Vitamin E Cancer Prevention Trial (SELECT) was intended to determine the effects of vitamin E, alone or with selenium, on prostate cancer.15 More than 35,500 subjects enrolled in the initial study, which showed a 17% increased risk of prostate cancer among those taking 400IU of vitamin E supplementation.16 Further analysis from SELECT determined that the high plasma phospholipid concentration of long-chain omega-3 polyunsaturated fatty acids also was associated with an increased incidence of prostate cancer.15 The specific omega-3 FA measurements analyzed in the blood were comprised of DHA, EPA and docosapentaenoic acid (DPA).
The retrospective case-controlled cohort design compared blood samples of 834 men diagnosed with prostate cancer (of which 156 had a “high-grade” diagnosis) to an age-matched subcohort of 1,393 men. Overall, there was a 43% increased risk of prostate cancer among those who had the highest level of omega-3 FA measurements in their blood. Men with the highest blood plasma level of omega-3 FAs had a 44% increased risk of developing “low-grade” prostate cancer, and a 71% increased risk of developing “high-grade.” Increased levels of blood serum linoleic acid (primarily comprised of omega-6 fatty acids) were associated with a decreased risk of “low-grade” prostate cancer.15
However, a closer look at the study raised several questions.
• Its original goal was to evaluate the relationship between prostate cancer and vitamin E, not omega-3 FAs.
• No other study has shown an increased risk of prostate cancer related to omega-3 FA supplementation.
• Specific variables with regard to the omega-3 FAs were not addressed. This included, but was not limited to, the type of omega-3 FA supplements taken, quantity of omega-3 FA intake, distinction between dietary intake and supplementation, and/or quality of omega-3 FAs intake.
• Red blood cell analysis of DHA and EPA is the conventional and acceptable marker for measuring omega-3 FA intake. Blood plasma evaluation may not yield an adequate assessment.
• Singular measurements were taken at commencement of the study.
• The data does not explain the relationship as cause and effect.
• Prostate cancer is associated with several contributing factors. The study accounted for some, not all.
• An intervention design, rather than a retrospective study, would have been more adequate to determine a definitive relationship between omega-3 FAs and prostate cancer.
• In some cases a digital rectal exam was conducted, but no biopsies.
Given our patient’s overall clinical picture, we suggested that he cease the use of omega-3 supplementation, but continue with an AREDS product that substituted lutein for beta-carotene.
1. Simopoulos AP. Omega-3 fatty acids in inflammation and autoimmune diseases. J Am Coll Nutr. 2002 Dec;21(6):495-505.
2. Harris WS. Fish oil supplementation: evidence for health benefits. Cleve Clin J Med. 204 Mar;71(3):208-10, 212, 215-8.
3. Roncone M, Bartlett H, Eperjesi F. Essential fatty acids for dry eye: a review. Cont Lens Anterior Eye. 2010 Apr;33(2):49-54.
4. Hodge W. Effects of omega-3-3 fatty acids on eye health. Evid Rep Technol Assess (Summ). 2005 Jul;(117):1-6.
5. Szymanski KM. Fish consumption and prostate cancer risk: a review and meta-analysis. Am J Clin Nutr. 2010 Nov;92(5):1223-33.
6. Terry P, Lichtenstein P. Fatty fish consumption and risk of prostate cancer. Lancet. 2001 Jun 2;357(9270):1764-6.
7. Chavarro JE, Stampfer MJ, Hall MN, et al. A 22-y prospective study of fish intake in relation to prostate cancer incidence and mortality. Am J Clin Nutr. 2008 Nov;88(5):1297-303.
8. Augustsson K, Michaud DS, Rimm EB, et al., A prospective study of intake of fish and marine fatty acids and prostate cancer. Cancer Epidemiol Biomarkers Prev. 2003 Jan;12(1):64-7.
9. Norrish AE, Skeaff CM, Arribas GL, et al. Prostate cancer risk and consumption of fish oils: a dietary biomarker based case-control study. Br J Cancer. 1999 Dec;81(7):1238-42.
10. Leitzmann MF, Stampfer MJ, Michaud DS, et al. Dietary intake of n-3 and n-6 fatty acids and the risk of prostate cancer. Am J Clin Nutr. 2004 Jul;80(1):204-16.
11. Stott-Miller M. Consumption of deep-fried foods and risk of prostate cancer. Prostate. 2013 Jun;73(9):960-9.
12. SanGiovanni JP, Chew EY, Agron E, et. al. The Relationship of Dietary -3 Long-Chain Polyunsaturated Fatty Acid Intake Inversely Associated With 12-Year Progression to Advanced Age-Related Macular Degeneration: AREDS Report No. 23. Arch Ophthalmol. 2008 Sep;126(9):1274-9.
13. The Age-Related Eye Disease Study 2 (AREDS2) Research Group. Lutein-Zeaxanthin and Omega-3 Fatty Acids for Age-Related Macular Degeneration The Age-Related Eye Disease Study 2 (AREDS2) Randomized Clinical Trial. JAMA. 2013 May 15;309(19):2005-15.
14. The Risk and Prevention Study Collaborative Group. n–3 Fatty Acids in Patients with Multiple Cardiovascular Risk Factors. N Engl J Med. 2013 May 9;368(19):1800-8.
15. Brasky TM, Darke AK, Song X, et al. Plasma phospholipid fatty acid & prostate cancer risk in the SELECT trial. J Natl Cancer Inst. 2013 Aug 7;105(15):1132-41.
16. Klein EA, Thompson IM, Tangen CM, et al. Vitamin E and the Risk of Prostate Cancer: Results of The Selenium and Vitamin E Cancer Prevention Trial (SELECT). JAMA. 2011 Oct 12;306(14):1549-56.
