 |
An 84-year-old woman presented to the office with a chief complaint of blurry vision in her left eye, which she reported had begun after she encountered a fall about one month prior to her visit. She said the issue had gradually become worse over the ensuing month, making her left eye’s vision poor. She did not report any pain. She denied systemic disease or allergies of any kind.
Clinical Findings
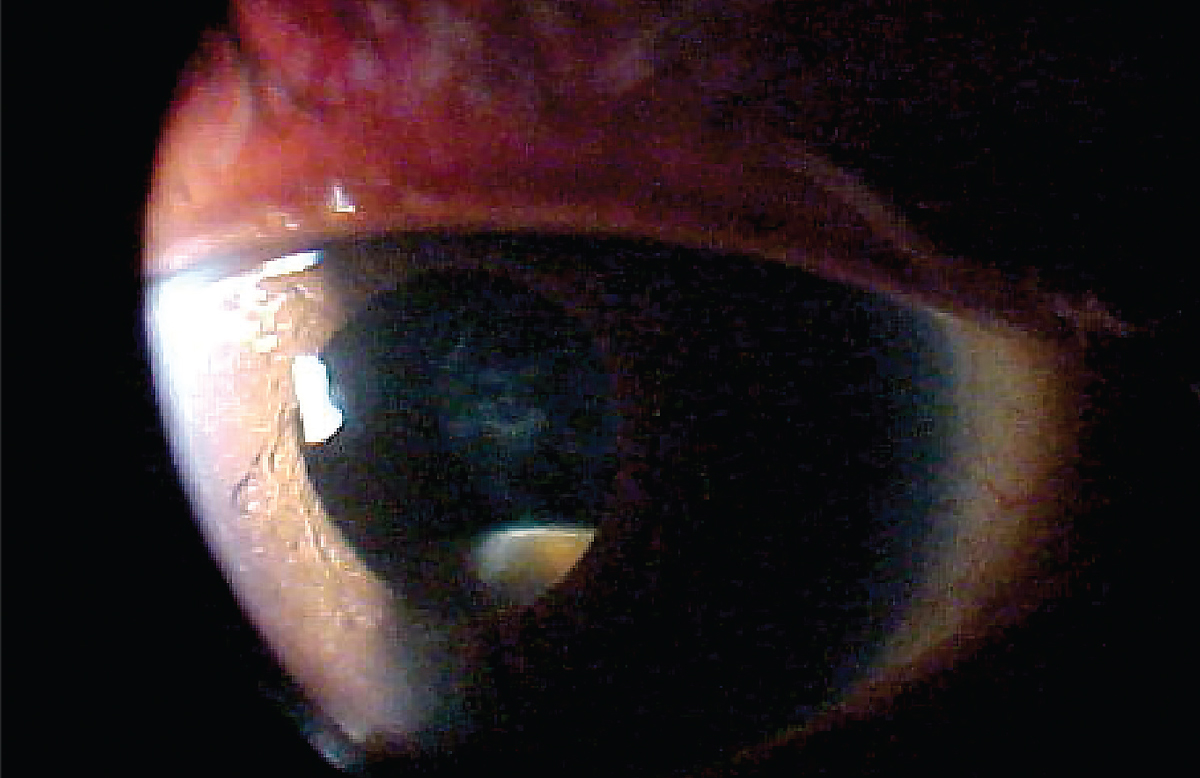
Her best-corrected entering visual acuities were 20/30 OD and 20/100 OS. Her external examination was unremarkable, with no evidence of afferent pupillary defect; the pertinent biomicroscopic finding is demonstrated in the photograph. Her Goldmann applanation tonometry measured 17mm Hg OU and her angles were grade 4 using the Van Herick angle estimation method.
 |
|
This was the patient’s presentation at the slit lamp. Does this explain her symptoms? Click image to enlarge. |
For More Information
Additional studies ordered in this case included B-scan ultrasonography to image the relevant ocular structures. Anterior segment OCT was helpful in the same way. Laser interferometry was completed to evaluate the foveal potential for acuity.
Additional health history questions were also asked to rule out any potential connection of the issue at hand to undiagnosed systemic disease, of which there were many of concern, chief among them pseudoexfoliation, amyloidosis, Marfan’s syndrome and Ehlers-Danlos syndrome.
What would be your diagnosis in this case? What is the patient’s likely prognosis?
Diagnosis
The history and clinical exam here support a diagnosis of traumatic crystalline lens subluxation. While this can occur in any patient, there are primarily three situations in which it is encountered. The first is a patient who has received significant blunt trauma to the eye, or in some cases to the head.1-5 The second is in patients with systemic conditions known to be associated with lens subluxation, such as Marfan syndrome, homocystinuria, Weill-Marchesani syndrome, Ehlers-Danlos syndrome, hyperlysinemia, amyloidosis with pseudoexfoliative disease, sulfite oxidase deficiency disorder, and hereditary ectopia lentis.6-9 The third scenario is a patient with a hypermature cataract in whom zonular support has been lost.10 In rare instances, crystalline lens subluxation can occur idiopathically and spontaneously.11-13 Other potential causes include ocular surgery, retinitis pigmentosa, congenital aniridia and vigorous eye rubbing.14-18
Lens subluxation commonly induces a visual disturbance that can range from mild to extreme. Monocular diplopia is a common complaint, particularly when the crystalline lens bisects the pupil.19 Displacement of the lens can also result in extreme refractive hyperopic or myopic changes, as well as induced astigmatism; in children, these changes can be amblyogenic.6 Occasionally, vision fluctuates as the patient alternates between the normal eye (phakic) and aphakic (subluxed) vision.20 In most cases, there is no physical sensation unless the lens physically blocks the pupil, leading to secondary angle closure pupil block glaucoma or iritis from an incident traumatic event.17,21,22 In acute secondary angle closure glaucoma an edematous cornea, blurred vision, headache, pain, photophobia, lacrimation, nausea and vomiting will be present. Open-angle glaucoma is also possible in cases of crystalline lens subluxation, with the primary mechanisms being traumatic damage to the anterior chamber angle (e.g., angle recession) or lens particle-induced inflammation.23
Examination demonstrates a displaced crystalline lens upon biomicroscopy. Using direct illumination, this is seen as an intrapupillary dark crescent against the convex edge of the displaced lens; often seen best with retroillumination, the dark crescent is replaced by a red reflex crescent that appears brighter than the adjacent lens. Dislocation of the lens may be up and out, down and in, down and out, nasal or temporal, or the lens may be completely displaced into the posterior or anterior chamber. The lens may also be “secluded” within the pupil. One may also observe phacodonesis (tremulousness of the lens due to loss of zonular support) and/or iridodonesis (tremulousness of the iris) as the patient makes small saccadic eye movements.11,17
The term subluxation generically implies a partial dislocation of an organ from its normal anatomical location. Crystalline lens subluxation describes a scenario in which the lens is displaced from its typical position within the anterior vitreo-hyaloid fossa. Ectopia lentis is sometimes used as a synonym for lens subluxation; however, this terminology is typically reserved for associated hereditary disorders (e.g., Marfan syndrome) in which the displacement is bilateral and symmetrical.6 The term luxation generically implies an organ is completely dislocated. When a lens is dislodged, such that it falls back into the vitreous body or posterior chamber or forward into the anterior chamber, the condition may be referred to as crystalline lens luxation.
Subluxation associated with trauma appears to be slightly more common than lens displacement associated with underlying systemic disorders.24,25 It is believed that the physical stretching and/or breaking of the zonules associated with traumatic insult is the mechanism by which subluxation occurs.25 This occurs as the eye is compressed in an anterior-posterior direction (such as with impact by a fist or other projectile) and the subsequent distention of the globe in the medial-lateral plane ruptures the zonular fibers.
Crystalline lens subluxation associated with congenital disorders varies in pathophysiologic mechanism, depending upon the individual condition. The direction of displacement in each case is characteristic but by no means completely diagnostic. Marfan syndrome is the most commonly encountered underlying condition in patients with crystalline lens subluxation. About 60% of these individuals demonstrate ectopia lentis.26 The typical direction of lens displacement in Marfan syndrome tends to be superior-temporal, but superior-nasal subluxation has also been documented.6,27 The underlying mechanism is believed to be abnormally constructed collagen vascular tissue and faulty lens zonules.
Typically, the subluxation associated with Marfan syndrome is non-progressive. Furthermore, since the zonules remain attached to the lens capsule, some degree of accommodation persists. Homocystinuria, a defect in amino acid metabolism, results in degeneration of the zonules with zonular rupture being the ultimate result.6 The characteristic displacement is inferior-nasal with cases that have been noted to luxate into the anterior chamber.6,9 Unlike in Marfan syndrome, accommodation is typically lost in homocystinuria and the subluxation may be progressive.9 Patients with Weill-Marchesani syndrome commonly exhibit microspherophakia, which is defined as a small, spherically shaped crystalline lens. The lens also lacks microfibrils around its equator, resulting in rupture of the zonules and a characteristic downward displacement of the lens.6,28,29 The microspherophakia combined with forward lens subluxation places the patient at increased risk for secondary angle closure with pupil block glaucoma.29,30
Two rare conditions that bear mentioning are ectopia lentis simplex and ectopia lentis et pupillae, both forms of hereditary ectopia lentis.6 Ectopia lentis simplex is believed to be inherited as an autosomal dominant trait, although there are no other associated systemic abnormalities. In this condition, the crystalline lenses are bilaterally and symmetrically dislocated superior-temporally, while the iris and pupil remain normal and intact. Ectopia lentis et pupillae is likewise an isolated congenital condition with autosomal recessive heredity.31 Features of this condition include enlarged corneal diameters, microspherophakia and corectopia. The lenses and pupils are displaced opposite each other in this bilateral condition.6,31
Prognosis and Management
A major concern with lens subluxation is the development of secondary angle closure glaucoma. Displacement of the crystalline lens introduces the possibility of firm apposition between the lens and the posterior aspect of the iris. When the pupil becomes obstructed, this is referred to as pupil block; iris bombé and secondary angle closure can result.21,29,32 Should a lens completely dislocate into the anterior chamber, one should be concerned about the lens possibly touching the cornea, irreversibly damaging the endothelial cells with subsequent chronic corneal edema and decompensation.11 Displacement of the lens into the anterior chamber can also result in a reverse pupil block angle closure glaucoma where the backward sagging pupil becomes sealed to the anterior hyaloid face of the vitreous.22
The management of patients with crystalline lens subluxation depends greatly on the severity of the condition and associated pathology. The degree of lens dislocation can be broadly classified into three categories: (1) minimal to mild lens subluxation, in which the lens edge uncovers less than 25% of the dilated pupil; (2) moderate lens subluxation, in which the lens edge uncovers 25% to 50% of the dilated pupil; and (3) severe lens subluxation, in which the lens edge uncovers greater than 50% of the pupil.33
Management tends to be conservative, especially for categories 1 and 2. The primary goal is optimization of vision through refractive correction.34 Improvement or elimination of monocular diplopia may be accomplished via the use of opaque contact lenses with small pupillary apertures. While it may be tempting to employ a miotic agent such as pilocarpine, this practice should be discouraged for long-term management. Pilocarpine can induce anterior rotation of the lens and exacerbate preexisting anterior subluxation secondary to zonulopathy, increasing the risk of pupillary block.12,35
Surgical intervention should only be considered when visual acuity becomes difficult to maintain despite best correction or in cases of anterior dislocation resulting in secondary glaucoma and/or corneal decompensation.34,36,37 For cases of posterior dislocation into the vitreous-posterior segment, intervention depends upon the status of the lens capsule. If the structure and capsule remain intact and no inflammation is detected, the condition can be monitored indefinitely.37,38 However, if persistent lens-induced (phacoanaphylactic) inflammation occurs or if the retina is compromised, then pars plana vitrectomy and lens extraction are indicated.2,37
Pupillary block with angle closure glaucoma ultimately warrants intervention with either laser peripheral iridotomy or lensectomy.39 First aid includes gonioscopy to confirm angle closure and fast-acting topical aqueous suppressant medications such as timolol along with brimonidine or apraclonidine. Anecdotally, I personally have had success by adding Travatan Z to the topical intervention. This was recommended to me by Drs. Melton and Thomas and I have had great success by employing the tactic. In cases that do not respond to topical-only therapy, oral acetazolamide (one 500mg tablet PO) or methazolamide (one 50mg tablet PO) can be dispensed. Oral osmoglyn or isosorbide should be reserved only for unresponsive cases.
Once the IOP has been lowered and the pupil block confirmed over by gonioscopy, low-dose pilocarpine can be dispensed to tighten the iris in preparation for the placement of surgical laser peripheral iridotomies. Unfortunately, this procedure rarely succeeds in managing the condition fully. Patients frequently require lens extraction with intraocular lens implantation. Phacoemulsification with posterior chamber intraocular lens and capsular tension ring (CTR) implantation has long been recognized as definitive surgical management of crystalline lens subluxation.40-42 More recently, a modified CTR and capsular tension segment has improved stability and intraocular lens centration via scleral-suture fixation.42
Finally, patients with “congenital” lens subluxation are rarely born with displaced lenses. The phenomenon typically develops during their life due secondary to the development of the predisposing systemic condition, such as Marfan syndrome.
In cases where there is suspected loss of zonular adherence (often in cases of hypermature cataracts) with risk of lens dislocation into the anterior chamber, pharmacological dilation should be avoided until a surgical consultation can be obtained. In any case of lens dislocation, there exists a strong possibility of pupil block and secondary angle closure glaucoma.
The mere fact that a lens is subluxed is not sufficient reason for surgical extraction. Here, the predominant consideration is function and cosmetics. Patients with crystalline lenses that dislocate into the vitreous are at risk for chronic and severe inflammation. This sequela may occur immediately or be delayed for years after the initial incident.
Dr. Gurwood thanks Dr. Al Kabat for his contributions to this case.
Dr. Gurwood is a professor of clinical sciences at The Eye Institute of the Pennsylvania College of Optometry at Salus University. He is a co-chief of Primary Care Suite 3. He is attending medical staff in the department of ophthalmology at Albert Einstein Medical Center, Philadelphia. He has no financial interests to disclose.
1. Izadi S, Stewart RM, Jain S. Bilateral posterior dislocation of the crystalline lens after a head injury sustained during a seizure. Emerg Med J. 2007;24(1):e6. |
