As refractive surgery continues to evolve, we have even more options to offer our patients. We"ve previously discussed the advances in wavefront-guided ablation (see "Wavefront Systems Available Today," August 2004, page 58). Three recent FDA actions offer our patients refractive options beyond the laser, especially keratoconus patients and patients with large amounts of myopia.
Intacs
Intacs intrastromal corneal rings (Addition Technology) are still available as a refractive alternative. However, when you consider that the cost of laser vision correction has declined and that custom wavefront-guided laser ablations offer greater predictability, few surgeons will implant the ring segments as a primary procedure.
Intacs received FDA approval in August for treating keratoconus under a Humanitarian Device Exemption. Intacs are finding their place more as a therapeutic treatment now.
For example, keratoconic patients have had Intacs implanted to provide structural support and reduce myopia and in some cases correct astigmatism.1 In one study in Beverly Hills, 74 eyes (50 patients) with keratoconus underwent a modified Intacs Procedure. A thicker ring segment was typically placed inferiorly, and a thinner segment was placed superiorly. Mean best-corrected LogMAR visual acuity went from 0.41 (20/50-1) peroperatively to 0.24 (20/32-2), an equivalent to two lines of improvement. Mean uncorrected LogMAR acuity went from 1.05 (20/200-2) to 0.61 (20/80-), or four lines of improvement.
Intacs" support characteristics are also shown to be beneficial in treating keratectasia following LASIK.2 In a Jersusalem clinic, for example, five eyes (five patients) were implanted with Intacs 17 to 32 months post LASIK. Mean manifest refraction spherical equivalent improved from 1.60D to 0.80D, and mean manifest astigmatic correction decreased from 3.90D to 2.46D. Corneal topography showed improved inferior steepening and less irregular astigmatism, and the mean inferior-superior asymmetry improved from 7.88D to 2.46D. Self-reported visual symptoms improved significantly in three of the patients and slightly in the remaining two.
 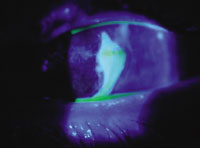 Images courtesy: Brian Chou, O.D. |
| Intacs can provide improved vision and structural support to keratoconus patients. This patient, however, experienced complications at day one post-op:The inferior segment extrudes out of incision site (left), and there is an associated epithelial defect shown by fluorescein (right). |
Phakic IOLs
Phakic IOLs are slowly becoming part of our armamentarium of refractive surgery.
Last month, the FDA approved the Verisyse/Artisan phakic IOL (Ophtec USA and Advanced Medical Optics) for use in patients with 5.00D to 20.00D of myopia. Verisyse, an iris-fixed anterior chamber IOL, is produced with a 5.0mm or 6.0mm optic, and has a treatment range of 5.00D to 20.00D of myopia.
Results have been promising. For example, in one study, 90 eyes (61 patients) underwent implantation with the Artisan lens or LASIK to correct 9.00D to 19.50D of myopia. Both options were found to be similarly effective, stable, and reasonably safe.3 Better uncorrected and spectacle-corrected visual acuity and contrast sensitivity, a lower enhancement rate, and exchangeability are the main advantages of Artisan lens implantation. Thirteen (72.2%) of 18 patients who received the Artisan lens in one eye and LASIK in the other preferred the Artisan lens to the LASIK, citing better quality of vision.
Also, the FDA Ophthalmic Devices Advisory Panel has recommended approval with conditions of the STAAR Visian ICL (implantable contact lens). The Visian is a foldable, posterior chamber, ciliary sulcus-based lens. It can treat myopia from 3.00D to 20.00D.
FDA clinical trials include data collected from 20 hyperopes with a mean preoperative spherical equivalent of +5.55D, and 65 myopes with a mean preoperative spherical equivalent of 8.42D, who were implanted with ICLs between November 1998 and March 2000.4 Postoperatively, 40% of the hyperopic eyes were 20/20 or better without correction, and 80% of the eyes were 20/40 or better without correction, with a mean spherical equivalent of +0.06D. One hyperopic lens was explanted, and no adverse events were reported.
Postoperatively, 52.31% of the myopic eyes were 20/20 or better without correction, and 92.3% of the eyes were 20/40 or better without correction, with a mean spherical equivalent of 0.31D. No lenses were explanted, and one patient was treated for angle closure.
This lens has been through many refinements, especially to decrease the risk of cataract formation due to the fact that the device can touch the crystalline lens. One study found that vaulting of the ICL is the primary source of cataract formation with phakic IOLs.5 The new design (V4) that received approval has a natural vaulting that substantially lowered the risk of cataract formation.
The potential of these lenses provides an option for patients who want refractive surgery but who are not LASIK candidates for various reasons.
Refractive surgery has gone through so many changes and refinements that it"s difficult to know what"s coming in the future. Lens implants, including phakic IOLs, will quickly change how we remedy very high levels of refractive errors, especially in patients with thin corneas.
J. Christopher Freeman, O.D., and Steven J. Dell, M.D., co-authored this article. Dr. Freeman is fellowship-trained in cornea and refractive surgery and is optometric director at Dell Laser Consultants in Austin, Texas. Dr. Dell is a surgeon, author, and lecturer on refractive surgery, and is medical director of Dell Laser Consultants.
1. Boxer Wachler BS, Christie JP, Chandra NS, et al. Intacs for keratoconus. Ophthalmology 2003 May;110(5):1031-40.
2. Pokroy R, Levinger S, Hirsh A. Single Intacs segment for post-laser in situ keratomileusis keratectasia. J Cataract Refract Surg. 2004 Aug;30(8):1685-95.
3. El Danasoury MA, El Maghraby A, Gamali TO. Comparison of iris-fixed Artisan lens implantation with excimer laser in situ keratomileusis in correcting myopia between -9.00 and -19.50 diopters: a randomized study. Ophthalmology 2002 May;109(5):955-64.
4. Bloomenstein MR, Dulaney DD, Barnet RW, Perkins SA. Posterior chamber phakic intraocular lens for moderate myopia and hyperopia. Optometry 2002 Jul;73(7):435-46.
5. Sanders DR, Vukich JA; ICL in Treatment of Myopia (ITM) Study Group. Incidence of lens opacities and clinically significant cataracts with the implantable contact lens: comparison of two lens designs. J Refract Surg 2002 Nov-Dec;18(6):673-82.
Vol. No: 141:10Issue:
10/23/04
