Scope Expansion SeriesRead the other articles featured in this series:
|
An area of scope of practice expansion in optometry that has perhaps seen the most success over the last decade or so is the right to prescribe oral drugs for ocular disease. Although state-by-state laws vary regarding permitted pharmaceutical agents, ODs in every state are now allowed to prescribe some form of oral medication (e.g., antivirals, antibiotics, antifungals, anti-inflammatory drugs, analgesics, antihistamines, steroids) to treat various eye conditions, giving you an opportunity to enhance your quality of care. This means that patients are able to access needed medications sooner and more conveniently from their primary eyecare providers. But these agents come with more serious adverse effects and that may create reluctance among those unfamiliar with their use.
 |
|
Obtaining a comprehensive patient medical history, including past and current use of medications, is critical to avoiding adverse events from potential drug interactions. Photo: Getty Images. Click image to enlarge. |
Status of Oral Med Laws for ODs
There have been several prescribing authority wins for optometrists over the last few years. Most recently, in October 2021, New York passed a scope of practice bill that allows optometrists to use oral pharmaceutical agents for the treatment of eye diseases, including antibiotics, antivirals and anti-glaucoma agents. With this new bill, which takes effect on January 1, 2023, New York joins 48 other states and the District of Columbia that allow optometrists to prescribe oral medications.
To break this statistic down further, here is the number of states that currently allow ODs to prescribe the following medications:
- Controlled substances: 48
- Oral glaucoma meds: 47
- Oral immunosuppressives: 46
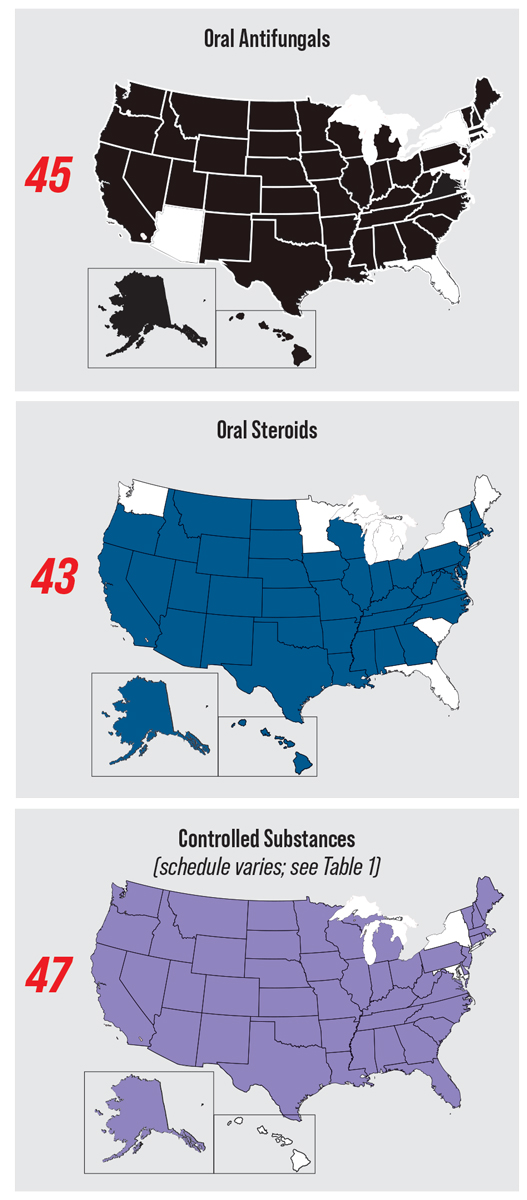
- Oral antifungals: 45
- Oral steroids: 43
- Hydrocodone: 36
ODs across the nation are experiencing firsthand the impact of these broadened prescribing rights on both their practices and patients. For Jill Autry, OD, RPh, who practices in Texas where optometrists recently gained the right to prescribe more oral medications (with the exception of Schedule 1 and 2 controlled substances), the biggest win has been the opportunity to start prescribing oral antivirals.
 |
|
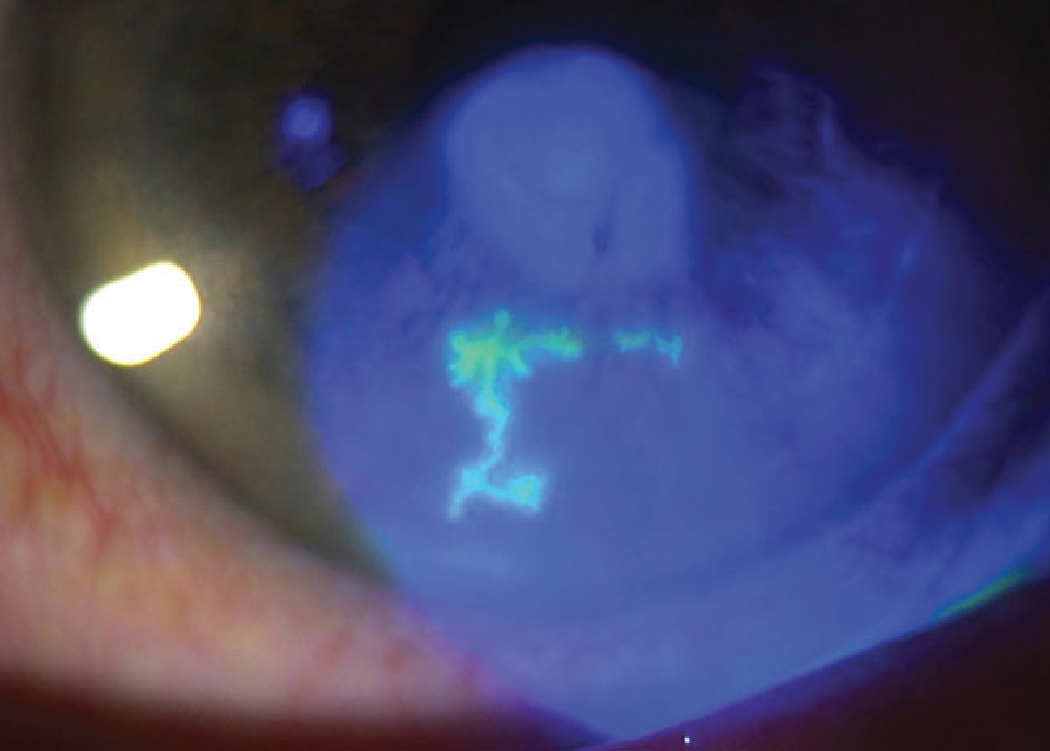
Antivirals are effective in treating several ocular infections such as herpes simplex keratitis. Allowing optometrists to prescribe these meds at the first sign of infection increases the likelihood of a positive outcome. Photo: Lisa Martén, MD. Click image to enlarge. |
“I am in a practice with ophthalmology, so I could always turn to them for the prescription, but it used to be very difficult for ODs in the community to try and get a primary care practitioner to prescribe or coordinate to send patients to an ophthalmologist for a prescription,” says Dr. Autry. “This was especially concerning after hours or on the weekend or when getting into an ophthalmology office could take several days when we know these medications are best started within 24 hours.”
To help ODs navigate additional opportunities to prescribe a variety of different oral medications, the fourth—and final—article in our scope expansion series will delve into the logistics of adding these services as well as cover clinical best practices to ensure optometrists have everything they need to successfully and confidently prescribe oral medications to manage patients with a wide range of ocular conditions.
Setting the Stage to Prescribe
As with any new clinical service you add to your practice, preparing to prescribe oral medications starts with ensuring you have a clear understanding of your state’s rules, laws and requirements.
In Florida, for instance, a Board of Optometry–approved 20-hour oral drug review course and examination is required before prescribing or administering any oral medication for an ocular condition, according to Jessica Steen, OD, an assistant professor at Nova Southeastern University’s College of Optometry.
“Prior to prescribing any controlled substance that is within the scope of state prescribing regulations, registration with the Drug Enforcement Agency is required and must be renewed every three years,” says Dr. Steen. “In certain states, specific continuing education requirements exist for those who carry additional certifications or registrations.”
 |
|
Patients with a lid infection like the one above, who has a hordeolum and preseptal cellulitis, may benefit from an oral antibiotic such as Augmentin (amoxicillin and clavulanate) or Moxatag (amoxicillin). Photo: Tracy Offerdahl, PharmD, and Greg Caldwell, OD. Click image to enlarge. |
You should check with your state optometric board to ensure you are prescribing within your scope, adds Jackie Burress, OD, of the Eastern Oklahoma VA Healthcare System. She also notes that certain medications may require lengthier training before you’re able to prescribe them at your clinic due to the strength of their effect and potential for misuse. This includes narcotics like hydrocodone used for treating painful chemical burns, abrasions or traumatic injuries, which ODs in several US states can now offer to patients.
“These are usually limited in the number of days that you can prescribe the medication to prevent abuse,” says Dr. Burress. “Also, ensure that you are checking the prescription drug monitoring program database before ever prescribing such medications to ensure a patient doesn’t have a pattern of drug-seeking behavior.”
Dr. Autry points out that steroids are part of another medication group a growing number of states allow ODs to prescribe that requires extra caution. Steroids have a high side effect profile that both patients and clinicians need to be aware of prior to starting the medication. She notes that knowledge of how to prescribe and follow patients on these agents is imperative to their health and safety.
 |
|
If a patient is relying on too many pain medications to alleviate their ocular discomfort, it is best to reassess the diagnosis and figure out an alternative game plan. Click image to enlarge. |
While all colleges of optometry provide the necessary education for prescribing oral medications, Dr. Burress notes that there are a plethora of resources available whether an OD is just starting to incorporate this service into their clinic or wants to enhance the care they already provide.
To confidently prescribe oral medications, Dr. Burress recommends brushing up on common conditions you see regularly. This includes reading CE articles and reviewing the Wills Eye Manual for the best and most up-to-date information, she says, adding that the Will’s Eye Manual provides excellent prescribing information for hordeola, preseptal cellulitis, herpes simplex and herpes zoster. Reaching out to your state board to see which educational and training resources they have available or know of is also a great place to start.
Aside from having the knowledge and skills to prescribe oral medications, the logistics of adding this service into practice are minimal, according to Dr. Burress. She describes that the process is the same as prescribing ophthalmic medications through your electronic health record system, which are then sent to the patient’s chosen pharmacy to be filled.
No matter which new service you integrate into practice, success depends on the involvement of the entire team. “Staff should already be well familiarized with the services and treatment options the optometrists at their office provide, and there should also be a triage system in place for ocular emergencies,” advises Dr. Steen. “When an OD decides to enhance their services, staff should be involved in the discussion to ensure accurate and effective communication with patients,” she says.
 |
|
ODs across the US are approaching near-universal access to oral medications, but there’s considerable variance within the controlled substance category. For more scope maps, see the first article in this series (May 2022). Click image to enlarge. |
Considerations and Best Practices
One key to successfully prescribing oral medications to your patients is to obtain a comprehensive medical history, detailed medication review (including supplements and vitamins), allergy history (including reaction) and review of systems, advises Dr. Steen.
“When prescribing any medication, including oral medications, it is important to get a comprehensive review of systems to uncover potential illnesses that may be contributing to the ocular conditions you are seeing and to determine if there are contraindications for specific medications that we may be prescribing,” says Christopher Wolfe, OD, who practices at Exclusively Eyecare in Omaha, NE. “Additionally, you would want to ask about previous medication allergies as well as current medications that are being taken.”
Like you would with any patient, conducting a complete clinical evaluation is imperative to determine a diagnosis and ensure that your proposed treatment strategy and medication choice is effective in managing the underlying cause of the clinical presentation, according to Dr. Steen.
“For instance, when choosing an effective oral antibiotic for a periorbital soft tissue infection, local resistance profiles, propensity for gastrointestinal upset and assessment of risk of harboring methicillin-resistant staphylococcus aureus should all be considered, in addition to potential risks identified through the medical history and medication review,” she says.
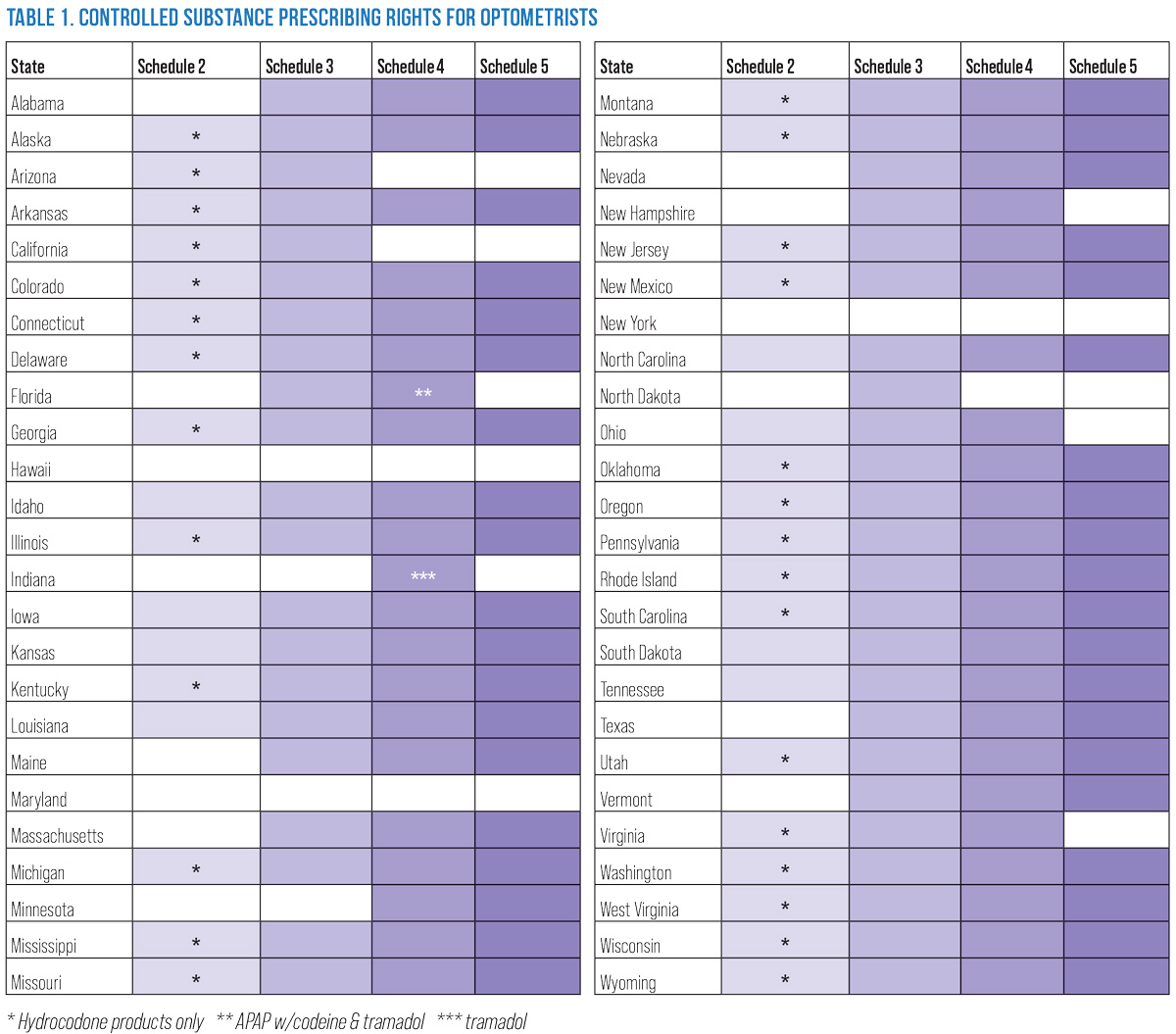 |
| Click image to enlarge. |
A drug interaction check program or app is also an important step to confirm that the proposed medication will not introduce a potentially harmful effect due to interaction with any current medications or supplements, suggests Dr. Steen, who also notes that many electronic medical records incorporate an interaction check into the electronic prescribing module. An alternative option is by accessing an outside system, such as that through Epocrates, which can be used online or via the company’s app.
“If an interaction is identified, assess the risk associated with the interaction and choose an alternative medication when possible,” says Dr. Steen. “If an alternative medication is not clinically appropriate, discuss the potential interaction and associated risks and benefits of your proposed treatment directly with the prescribing physician of the medication of concern. Depending on the physician’s availability and the urgency of treatment, a local pharmacist will also be able to provide decision-making support.”
Engaging with the patient throughout the entire process is another key component and the best way to make sure they’re satisfied with your care. Have a discussion with each patient before starting them on oral medication where you cover the anticipated effects—both positive and negative—as well as the potential adverse effects and what the patient should do if they occur.
“A clear understanding of expected effects of a medication can save the patient and prescriber from an additional unnecessary emergency appointment or save the patient from consequences of untreated disease or disease progression due to self-discontinuation of the medication,” explains Dr. Steen. “Every prescribing decision requires a careful evaluation of potential risks and benefits of treatment, and good adherence to therapy relies on a patient being engaged and well-informed regarding their therapy.”
It’s also important to take the patient’s insurance and financial situation into account when ordering medications, notes Dr. Burress. “Many times there is a less expensive option if that is what’s needed for the patient to improve their compliance,” she points out.
Gain Confidence in Your Prescribing SkillsAdding any new service into clinical practice can feel daunting, and oral medication prescription is no exception. An abundance of choices coupled with potential side effects and drug interactions can add another layer of complexity and potential stress to clinical practice. However, that doesn’t have to be the case. ODs have the knowledge and skills to prescribe oral medications to their patients. Confidence will increase as you prescribe more oral medications and you experience the clinical benefits of that prescription, says Dr. Wolfe, while suggesting that ODs can reduce their anxiety around this service by initially limiting oral prescriptions to the management of one area or medication class. A good place to start would be for eyelid conditions. “These are relatively common, typically very amenable to oral antibiotics and there are many resources (like the AOA’s Clinical Practice Guidelines) that can provide a stepwise approach as to what antibiotic would be best and what options are good when the first-line option is contraindicated,” he explains. Get comfortable with three to five medications that you use routinely and know their side effects, dosages, what to do if the treatment isn’t working, and so on, suggests Dr. Autry. “Just get your feet wet and expand as you go. It’s really pretty simple given we often are using the same medications over and over.” Familiarity will neutralize any anxiety over time. “Even the ophthalmologists I work with have standard medications they use with standard dosages and standard clinical uses. I saw this as a pharmacist as well across all types of medical practices,” Dr. Autry adds. “Everyone gets comfortable with certain medications in certain conditions with changes based on things like pregnancy, allergies and side effect profiles. If they can do it, so can you.” Other tips to help you get comfortable prescribing oral medications include:
|
Dosing Common Oral Meds
Given the number of available drugs, prescribing oral medications may feel overwhelming at first; however, for most eyecare issues, Dr. Autry notes there are standard medications that can be used. “As long as you check for allergies, pregnancy and severe hepatic and renal disease, you can usually prescribe the same five to seven oral medications,” she says. “For most lid infections, I use amoxicillin (Moxatag) 875mg BID for adults, and for suspension in children, I use 20mg to 40mg/kg/day.”
Augmentin (amoxicillin and clavulanate) 875mg can also be prescribed to adults or children with bacterial infections using the same dosing strategy as for amoxicillin; however, she notes that this isn’t needed as much today since most individuals are vaccinated against Haemophilus influenzae.
If a patient is allergic to penicillin, Dr. Autry opts for doxycycline (Monodox) 100mg (contraindicated for children or nursing/pregnant patients) BID PO or Septra DS (sulfamethoxazole-trimethoprim) BID. The latter should not be used in patients allergic to sulfa or those who are nursing or pregnant, but there is a suspension for children, she notes.
“I know a lot of ODs like Keflex (cefalexin) or Z-Pak (Zithromax, azithromycin), but these don’t always fix severe infections, and Keflex resistance is increasing,” she says. “Oral ciprofloxacin (Cetraxal) has almost no gram-positive coverage anymore, so I avoid it in cases of lid disease. Levaquin is an option but has its own possible side effects and is expensive.”
When considering pain medications, Dr. Autry typically recommends ibuprofen and/or acetaminophen. Together, the two have shown to be equivalent to Tylenol #3, she notes. “I tell patients to take 400mg ibuprofen (two of the OTC 200mg tabs) and one 500mg acetaminophen (extra strength Tylenol).”
ODs should be careful when using ibuprofen or other nonsteroidal anti-inflammatory drugs in patients with an aspirin allergy, cautions Dr. Autry, who adds that she prefers acetaminophen. If an OD finds they are using a lot of oral pain medications, she advises that they may need to rethink the patient’s diagnosis or seek a second opinion.
“Most ocular issues that cause pain can be handled with topical options like bandage contact lenses, cycloplegic agents or topical steroids,” Dr. Autry explains. “I don’t give pain medications to bacterial keratitis patients, as I need to know if they are feeling better on the antibiotic regimen to know if I am on the right track. The most I will do for them is cycloplegia and never, ever a bandage contact lens.”
Oral steroids should be used with care, particularly among older patients and those with gastrointestinal issues or diabetes. In most cases, Dr. Autry has found a Medrol (methylprednisolone) dose pack to be effective, which has its own taper schedule. When prescribing this to her patients, she tells them to take all six tablets in the morning with breakfast the first day, five tablets the next day with breakfast, and so on for the six days of therapy. She notes that this regimen follows the normal morning peaks of cortisol levels and also helps with patient compliance.
“This is a very common recommendation I saw as a pharmacist from non-emergency care practitioners such as primary care physicians and rheumatologists,” Dr. Autry says. “Otherwise, if using oral steroids, you have to taper appropriately. I recommend OTC Zantac (ranitidine), Pepcid (famotidine) or Prilosec (omeprazole) to protect the stomach with all steroid prescriptions.”
Oral antivirals are typically well-tolerated and cause few or no allergic reactions or side effects. Additionally, these agents are pregnancy and nursing safe, Dr. Autry says. For herpes zoster, she typically prescribes 1g valacyclovir (Valtrex) TID. In cases of herpes simplex (periocular infections and dendritic or disciform infections), her standard prescription is valacyclovir 500mg TID.
There are other uses for agents like this, she notes, such as Bell’s palsy (1g TID) and herpetic uveitis (500mg TID) as well as prevention of recurrent simplex after multiple infections (500mg valacyclovir QD to QOD long-term). According to Dr. Autry, there is no practical reason to use acyclovir (Sitavig or Zovirax) any more since it has to be given several times per day. Valacyclovir works better and has been generic for some time, she adds.
Once an OD has determined a diagnosis and the appropriate treatment strategy, including medication, dose, frequency, duration and directions for use, Dr. Steen notes that it is helpful to return to the medical history and current medications to confirm their completeness with a specific focus related to possible adverse effects of the proposed medication before sending the prescription to the pharmacy.
“For example, before prescribing azithromycin, confirm the absence of allergy to the medication, absence of cardiac arrhythmia, heart failure and liver disease due to known adverse effects and contraindications,” she elaborates. “When prescribing any drug for a female patient of child-bearing age, re-confirm that they are not currently pregnant or lactating, and for all antibiotic prescriptions, if the patient is currently taking an oral contraceptive, advise the patient to use an alternative method of contraception during and for seven days following treatment.”
At this point, the OD should outline a clear follow-up schedule and ensure that emergency contact information has been provided to the patient, according to Dr. Steen. It’s also important to remember that while there is a standard approach to oral medications that can typically be followed, every patient has a unique history and needs.
“The diagnosis, treatment and management of ocular diseases and disorders is the core of providing primary eyecare and is central to optometry,” says Dr. Steen. “There is no ‘one size fits all’ approach to the management of any individual ocular condition. Timely and appropriate treatment of ocular disorders relies on an individualized approach which starts with an accurate diagnosis and centers on careful consideration of patient, condition and medication-specific features.”
 |
|
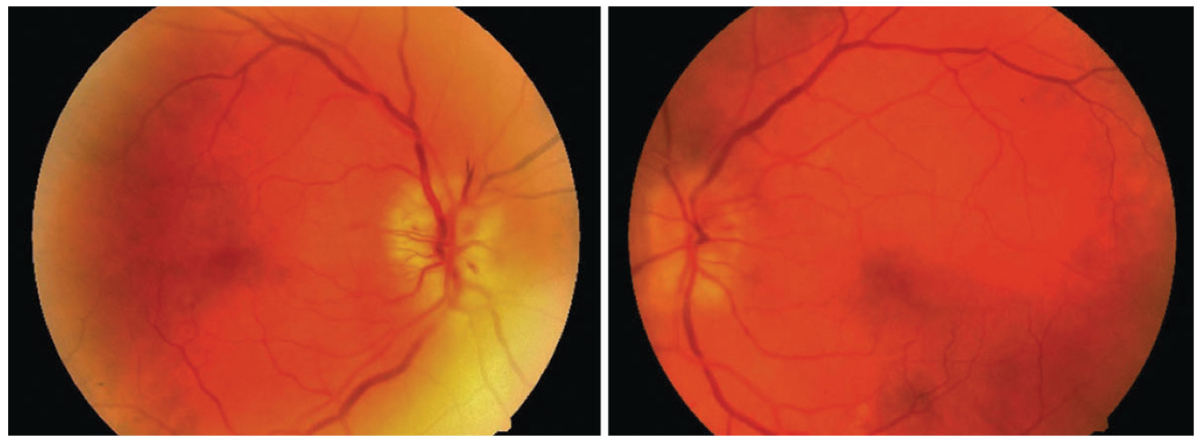
This patient’s anterior ischemic optic neuropathy was effectively resolved with a systemic steroid; however, the patient had diabetes, which worsened secondary to steroid treatment. It’s important to be aware of this contraindication for those with this comorbidity. Photo: Jason Duncan, OD. Click image to enlarge. |
Leading Primary Eyecare
Throughout this scope expansion series, we have explored the critical role optometrists play in a variety of services and procedures, but the common message has been the important position ODs hold as primary eyecare providers. Whether we’re talking about incorporating oral therapies, removing lid lesions, injecting steroids, using lasers or managing glaucoma (the key topics covered in this series), taking advantage of new or existing practice rights is vital to continue growing in your career and to promote the well-being of your patients.
Ongoing legislative wins across the country are making it possible for more and more ODs to practice to the full extent of their expertise and embrace their leading role in eyecare. It’s up to every OD—as well as the optometric community as a whole—to meet this challenge head-on.
“If you are not able to meet all of your patients’ needs and offer them well-rounded care, they may seek care where they don’t feel they are limited,” says Dr. Burress. “Prescribing oral medications places you in the patient’s mind as their primary eyecare provider who can take care of not only their refractive needs, but ocular health needs as well.”
“With the decreasing number of ophthalmologists and increasing number of patients needing care, optometry has to step up and manage medical conditions that in the past may have gone to someone else,” urges Dr. Autry, adding that politicians also have to do their part to expand optometric scope of practice. “Many of our colleagues in optometry have spent their own time, sweat and tears to get us increased scope across the country. Don’t let their hard work go to waste by not taking advantage of the expansion in your state.”
