 |
When Marc and I look for topics for this column, we often circle back to questions such as, “With what concepts do our students most often struggle?” or “What topic would be a useful refresher?” Since we’re all lifelong students, it makes sense to us that our fellow practicing docs might also be interested in discussions tackling these topics. One topic that has popped up rather often is that of knowing when and how to diagnose amblyopia.
We’ve all learned that amblyopia is a “diagnosis of exclusion,” but what does that really mean? I recently heard a colleague describe it as not only a diagnosis of exclusion, but also of inclusion (many thanks to Dr. Morgan Ollinger for the phrase!), and I love this way of putting it; not only do we as practitioners need to rule out the bad stuff, but we have to make sure that there is a reason for the reduced function (most often visual acuity) that we see before we call something amblyopia. We offer here a refresher of those findings that are required for the diagnosis to be made.
Amblyogenic Factors
To understand these, it makes sense to remind ourselves of what amblyopia is—and what it isn’t. As commonly understood, amblyopia is “an acquired unilateral or bilateral decrease in visual acuity for which no obvious structural or pathologic causes can be detected.”1 There are many other decreases in function due to amblyopia in both the worse- and better-seeing eyes, but these will have to be addressed in another column. Amblyopia is the result of some disruption to the developing visual system during infancy or early childhood and therefore will not be the result of injury or insult later in life. For example, a traumatic cataract at age 35 brought on by a car accident may cause a decrease in acuity, but that decrease is not considered amblyopia. There are several major classifications of amblyopia—organic, psychogenic and functional—with the latter being the category that we will discuss here. To break things down even further, within the classification of functional amblyopia, we have refractive (either anisometropic or isoametropic), strabismic and deprivational subclasses.
The most important thing that we need to do as practitioners when we have a patient with decreased acuity is answer the “why?” question. Why is the acuity reduced? Do we have an obvious reason—for example, some readily visible pathology? Is there uncorrected refractive error? Has the patient ever been able to achieve better acuity in the past? There are numerous other questions that can be asked, and we tend to go through a bit of a mental checklist during our exams that answers many (if not most) of them. We perform chair skills, we refract, we carefully assess ocular health. Once we do these things, we often are able to help the patient achieve good acuity or at least have the answers we need to explain any remaining deficits.
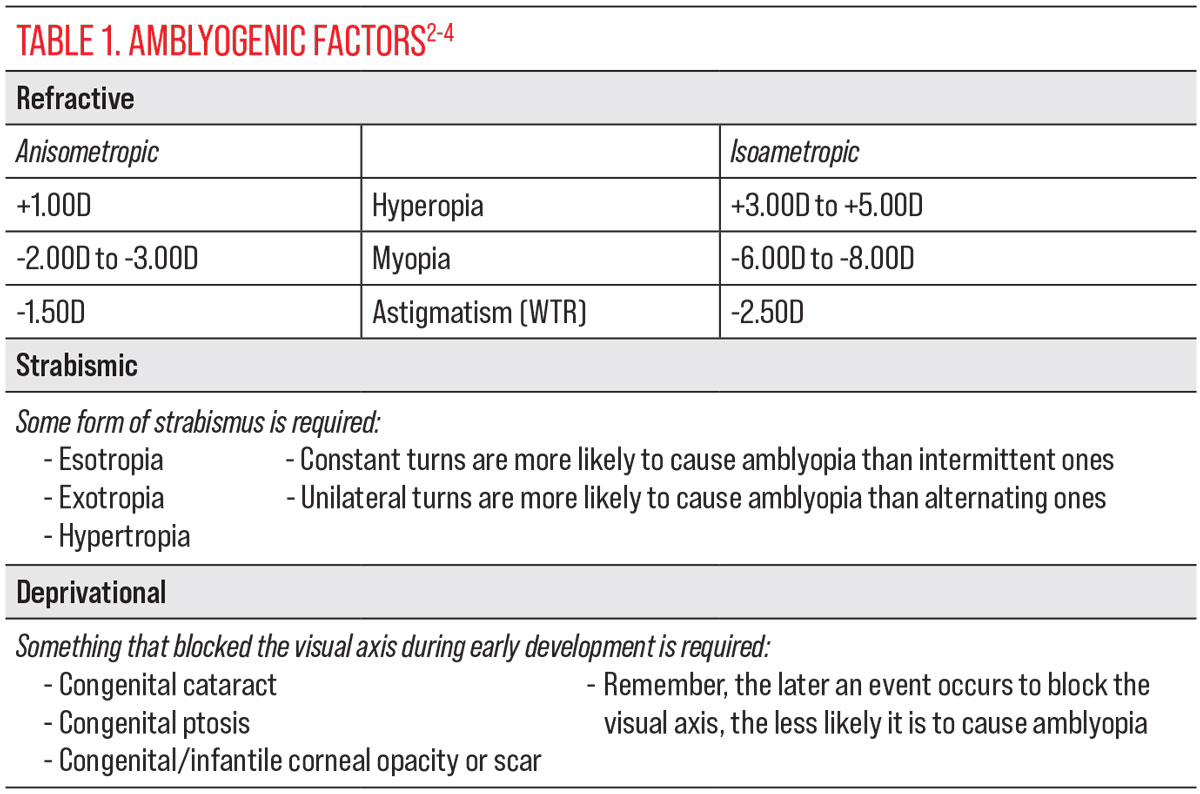
But what about when we don’t have an explanation? Are we looking at amblyopia? For each of the above-mentioned categories (strabismic, refractive or deprivational), there are certain findings that we need to see if we are going to diagnose amblyopia. Since I am an organizer, I love having things displayed logically as well as creating lists and tables, so Table 1 puts the amblyogenic factors all in one place for easy reference. Without one or more of these findings, we can’t diagnose amblyopia, so keep digging for answers. Even with a factor or two showing up in your exam data, remember that not every patient will have reduced acuity as a result. All findings should be evaluated within the broader context of the whole patient. Let’s look at a few of these cases to illustrate the importance of the amblyogenic factors.
 |
| Click image to enlarge. |
Case 1
This patient is a 15-year-old girl who presented to our clinic with the chief complaint of longstanding blurry vision in both eyes. She reported that she had glasses at some point in the past (she couldn’t remember when), but they were lost. As this was her first visit with us, we had no record of any previous prescription. Entering unaided acuities were 20/80 OD and 20/60-1 OS with pinhole acuity of 20/50 in each eye. At near, she achieved 20/32 OD and 20/40 OS. Refraction revealed moderate compound hyperopic astigmatism (+3.50 -1.25x180 OD, +3.25 -1.00x010 OS), which gave a best-corrected acuity of 20/50 in each eye. Cycloplegia showed additional hyperopia (+6.50D OD, +5.50D OS), with similar cylinder. Pupils, color vision and confrontation visual fields were all normal, as was ocular health with dilated examination.
Is this amblyopia? We have ruled out obvious retinal or optic nerve pathology and we have an amblyogenic factor in the refractive findings. Given this, we were comfortable prescribing—a trial frame of +3.50 -1.00x180 OD/OS showed 20/25 OU visual acuity—and diagnosing binocular dysfunction, but we held off on calling this bilateral refractive amblyopia for the time being. Why? She needs to adapt to her new prescription and show us that this isn’t simply a case of uncorrected refractive error. The patient is scheduled for a two-month follow-up in order to assess her progress.
Case 2
A 13-year-old boy came to us with a previous diagnosis of refractive amblyopia. He had been diagnosed with the condition at least two years prior and had been wearing glasses and patching. He had also begun a program of vision therapy with limited improvement so far. Entering visual acuities with his current prescription (+2.50D OD, +1.75D OS) were 20/50-1 OD and 20/20+3 OS. Refraction at the most recent visit showed little change; an updated prescription of +3.00D OD, +2.00D OS was released, with best-corrected acuity of 20/40 OD, 20/20+3 OS. Based on this information, I was skeptical that we really had a case of amblyopia—the difference in hyperopia is technically large enough, but it seemed like too much of an acuity deficit for only a 1.00D difference—so we went digging for more information.
As with the patient in Case 1, pupils, color vision and confrontation visual fields were all normal. Ocular health with dilated exam was also negative for any obvious pathology. Stereo testing was reduced, however, and cover testing showed 10 exophoria at distance and near. Near point of convergence was quite receded, to 11cm/17cm on three attempts. The patient suppressed the right eye on both near base-in and near base-out vergence testing. After all of this, a repeat cover test was performed, since something still didn’t add up—a phoria is not amblyogenic. This time, a small but constant right exotropia was found, of approximately eight to 10 prism diopters. Aha, now we had an explanation! While the anisometropia was only barely enough to cause refractive amblyopia OD, the presence of a constant right XT provided the amblyogenic factor that allowed us to diagnose strabismic amblyopia in the right eye. With a shift in therapeutic activities and goals in his vision therapy program, he has started making much better progress.
 |
|
The most common complaint related to amblyopia is blurry vision. Photo: Seth Taub. Click image to enlarge. |
Case 3
This patient actually just presented to clinic this morning, as I’m finishing this column. This 15-year-old girl complained of longstanding distance blur in both eyes with her current glasses. Her entering acuities were 20/60 OD, 20/40 OS; as with our other two patients, pupils, color vision and confrontation visual field were normal. Upon refraction, we found +3.00 -5.00x010 OD and +3.50 -6.00x170 OS, which was similar to what she was already wearing. A new prescription was given since her old frame was bent and her lenses were badly scratched. Her best-corrected visual acuity did not change much and her near acuity was also decreased to approximately 20/50, so much of the typical near-point testing was deferred to a follow-up in eight weeks, although ocular alignment was shown to be grossly intact on cover testing with a non-accommodative target. Ocular health with dilation was normal.
So, what do we have in this case? Can we call this amblyopia? Unlike with Case 2, this patient did not come in with a diagnosis in place. She certainly has an amblyogenic factor with such high astigmatism, and the level of reduction in acuity makes sense, except for the fact that she has been wearing a similar prescription for some time. Several questions arise: Has her wear time been consistent with her old prescription? Did she ever truly adapt to it? Is there any pathology that we were unable to find today? (I’m pointing at you, cornea! A topography is warranted with this much astigmatism.)
Given that we still have unanswered questions such as these, we can’t be certain at this time that this is truly amblyopia. Remember, we have to exclude all of the potential pathological findings first, as well as determine whether the patient is in their best refractive correction. For this patient, while we did assess suspected refractive amblyopia OD/OS, we also referred her for a corneal evaluation and set up a follow-up exam. We will re-evaluate her acuity and binocularity at that time, as well as the findings from the corneal evaluation. If she adapts well to her glasses and still has reduced visual acuity—and assuming that her corneas are determined to be otherwise healthy (e.g., free from keratoconus)—we can feel much more comfortable calling this amblyopia.
Takeaways
We’ve talked a bit about what amblyopia is and have looked at several cases as examples. As I mentioned at the beginning, though, it’s vital to remember what amblyopia isn’t. It is not a catch-all, a diagnosis to be used when you aren’t sure what has caused a patient’s reduced acuity. Calling unexplained acuity loss “amblyopia” is a recipe for disaster for the patient when that isn’t accurate (not to mention a significant potential legal issue for the doctor), so we have to guard ourselves against the fallback of using “amblyopia” and not pursuing the situation further. Make sure you rule out pathology, make sure that you have at least one amblyogenic factor before calling something amblyopia (some patients have several) and make sure you follow up appropriately. Your patients will benefit from your attention to detail.
Dr. Taub is a professor and co-supervisor of the Vision Therapy and Pediatrics residency at Southern College of Optometry (SCO) in Memphis. He specializes in vision therapy, pediatrics and brain injury. Dr. Schnell is a professor at SCO and teaches courses on ocular motility and vision therapy. She works in the pediatric and vision therapy clinics and is co-supervisor of the Vision Therapy and Pediatrics residency. Her clinical interests include infant and toddler eye care, vision therapy, visual development and the treatment and management of special populations. They have no financial interests to disclose.
1. Rutstein RP, Daum KM. Anomalies of binocular vision: diagnosis and management. Mosby. 1998:p. 7. 2. Scheiman M, Wick B. Clinical management of binocular vision: heterophoric, accommodative, and eye movement disorders. 4th ed. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins. 2014. 3. Lyon DW, Jensen KA. Amblyopia: diagnosis and treatment. In: Schnell PH, Taub MB, Duckman RH, eds. Visual Development, Diagnosis, and Treatment of the Pediatric Patient. 2nd ed. Wolters Kluwer/Lippincott Williams & Wilkins. 2020. 4. Press LJ, Tea YC, Lyon DW. Amblyopia: a microcosm of visual disorders. In: Press LJ, Taub MB, Schnell PH, eds. Applied Concepts in Vision Therapy 2.0. Optometric Extension Program Foundation. 2022. |
