Many practitioners panic when they see a child on the schedule. Have no fear! Children are often easier to examine than adults once you get some practice under your belt. Getting comfortable with examining them allows practitioners to serve an important need in the medical community. It is crucial to perform eye examinations on children to ensure their visual system is properly developing. Visual acuity, stereopsis and oculomotor skills develop rapidly throughout childhood. It is critical to catch any potential barriers to normal visual development as early as possible. The American Optometric Association (AOA) recommends a child’s first eye exam occur between six to 12 months of age. Subsequently, asymptomatic or low risk children should be seen at least once between three and five years of age and before beginning first grade. Annual eye exams are recommended for all children between ages six and 18.1 This can also help build your practice, as many parents and other family members will often seek care from you once you have successfully examined their child.
 |
|
Retinoscopy performed out-of-phoropter using a skiaskopy bar. Click image to enlarge. |
Throughout a child’s development there are key visual milestones that optometrists look for, which are reflected in our chosen examination procedures. An eye exam on an infant will be very different than the eye exam we perform on a typical schoolchild. During the initial eye exam between six and 12 months of age, be concerned about significant abnormalities in the visual system such as high refractive error, binocular vision disorders, strabismus or presence of ocular disease. These examinations are completely objective and generally very short, focusing on retinoscopy, cover test, pupil and extraocular muscle function and anterior and posterior segment health. In toddlers and preschoolers, we can begin getting some subjective feedback. The exam will still mainly consist of objective measurements and ensuring the child’s visual development is appropriate for their age. When examining school-aged children, we need to ensure they are meeting the visual demands required for school. This should include a full assessment of refractive error, binocular vision and ocular health.
Keep It Fun
Eye exams on children need to be fast-paced and fun! The more fixation targets you can acquire, the better. Switching the target frequently increases child engagement and move the exam along faster, as well as ensuring that the patient is focusing on it. Fixation toys do not need to be an expensive investment. A simple rubber duck can be used as a fixation target on your transilluminator. Spinning light toys and finger puppets from local toy stores are very useful as well. Small, detailed stickers work well to create fun accommodative targets for patients. Nail stickers or small stickers can be placed on popsicle sticks and contain the perfect amount of fine detail to act as an accommodative target. Kids YouTube or a favorite television program or movie on a device can serve as an excellent tool during retinoscopy. During the ocular health evaluation, a parent or assistant can hold a phone or tablet at different locations to direct fixation and allow you to easily examine your patient.
 |
|
Using a variety of fixation targets helps engage the patient. Click image to enlarge. |
An investment in some additional equipment might ensure a successful pediatric examination. When examining young children or patients with developmental disabilities, Snellen or ETDRS targets are often not ideal for measuring visual acuity because they rely on letter recognition. Teller Acuity Cards use a forced choice preferential looking technique and are a quick way to evaluate visual acuity in infants and very young children. Teller cards are commonly used in patients less than one year of age, but may be used to evaluate acuity in children 36 months and younger, and also older children or adults with developmental disabilities.2 Cardiff cards contain vanishing optotypes of familiar shapes and are ideal for children ages one to three, who may not attend to the gratings on Teller cards.3 The technique for testing acuity is forced choice preferential looking and the test can be performed at 50cm or one meter.
Using Lea symbols or an HOTV chart can be helpful for testing children ages three to seven years. Lea symbols consist of four calibrated shapes that are easily recognized by most children. A matching card or matching puzzle helps with testing acuity in children who are shy or do not know their letters. HOTV testing also uses a matching card, which allows for testing even in children who do not know their letters. The Vision in Preschoolers study group found that both Lea and HOTV can be used in most three- to five-year-old children, but three-year-old children had more difficulty with the HOTV chart.4 Both Lea and HOTV charts are commonly included in electronic acuity chart programs making them easy to use in most clinics.
Stereoacuity is a useful test in pediatric eye examinations because you can gain insight into different aspects of the child’s visual system with one test. When evaluating stereoacuity, it is important to remember that a random dot stereogram, or global stereopsis test, requires the patient to be bifoveal to appreciate the random dot shape. Local or lateral disparity stereopsis tests, such as the Wirt circles or the fly test, have monocular cues, so even patients with constant strabismus (or patients who are not bifoveal) can often correctly identify some of the coarser degrees of stereopsis in this test. Random dot stereopsis can be reliably tested even in young children.
Most preschool aged children without strabismus or a high degree of uncorrected refractive error or unequal visual acuity are able to successfully complete the test, demonstrating that the child has normal binocularity (no constant strabismus) and likely does not have high degrees of uncorrected refractive error or poor acuity in one or both eyes.5,6 Stereoacuity develops in the first six months of life, and most children between five and six months of age have been shown to have stereopsis.7
The Pediatric Assessment of Stereopsis with a Smile (PASS) test is an excellent tool to assess stereoacuity in young children. This test can easily be administered by the doctor or support staff and uses a preferential looking technique, which makes it easier when testing younger children.8 The Preschool Stereo test has a matching card, which makes it easy to test preschool aged children, and the Randot butterfly has a large stereopsis butterfly target and is also easy to use in young children. It is helpful to prompt the child to look for the smiley face that is “popping out,” and there is a demonstration card available to help small children know what they are looking for.
Many parents seek care because they are concerned their child may have a color vision defect. In younger children, traditional measures of color vision can be cumbersome and time consuming. The Color Vision Testing Made Easy (CTVME) is a much more suitable test for them. It consists of child-friendly shapes, can generally be completed in 60 seconds or less and can accurately identify color vision deficits in children as young as five years old.9 Color vision defects are commonly worrisome to parents. It is important to counsel parents that while colors may not appear normal to their child, it should not have severe implications for quality of life, but some limitations—such as career limitations— may exist.
 |
| Click table to enlarge. |
Testing Sequence
Children have limited attention spans so the key to successfully examining this population is to keep the exam moving quickly and prioritizing certain exam elements. Unlike traditional eye exam sequencing, in infants and young children, visual acuity is not the first test to be completed. Visual acuity can be a challenging test, and it may be frustrating for the child. Additionally, some children may become upset when an eye is occluded during monocular acuity testing. For this reason, we recommend the following examination sequence for young children: entrance testing (confrontation visual fields, extraocular motility and pupil function), Hirschberg testing, stereopsis testing, color vision testing, retinoscopy, visual acuity, IOP and dilated fundus evaluation with cycloplegic refraction.
Depending on the child you are working with and their age, it may not always be possible to complete the entire exam in one visit. Do not be afraid to suggest completing the exam on a separate visit if you notice a child is becoming agitated or upset. Parents are usually understanding and willing to bring the child back to get accurate testing data. When scheduling young children, it is also important to avoid nap time or meal time when possible.
 |
|
Teller acuity (preferential looking) performed on an infant. Click image to enlarge. |
In older children, ages six to 13, the exam sequence is similar to an adult exam, with the addition of binocular vision testing. Screening school-aged patients for binocular vision disorders is important, and even patients who do not have symptoms consistent with a binocular vision disorder should have basic screening, as most children do not realize their symptoms are associated with their eyes or may avoid near work to avoid symptoms.
Case History
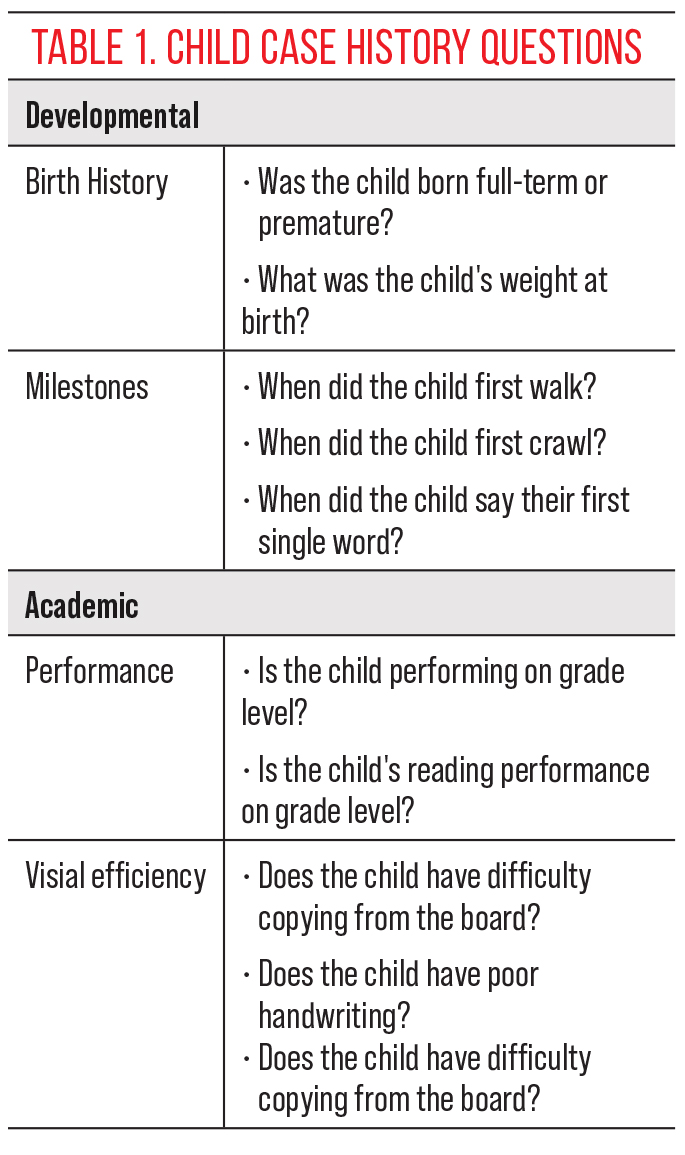
To maximize children’s attention in the exam room, it is best to have parents fill out information on developmental and academic history prior to the examination. There are some important milestones in development you would like to inquire about with parents (Table 1).
The College of Optometrists in Vision Development Quality of Life survey can also be used as a screening tool prior to examining children ages six and up. It has been found to be a reliable screening tool to identify visual symptoms in children who may have a vision disorder.10
Refractive Error Assessment
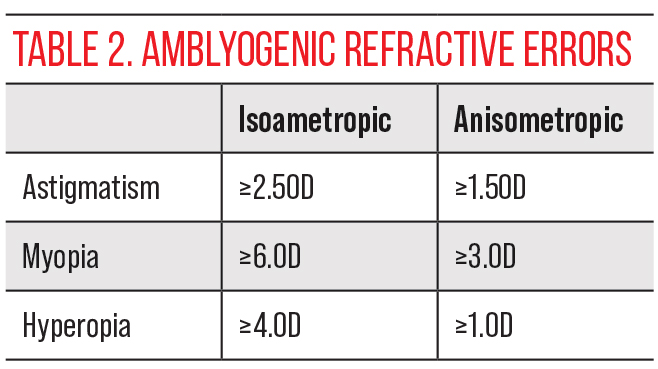
When examining children, place greater emphasis on objective testing measurements. Retinoscopy is crucial to look for the presence of a significant refractive error or anisometropia and to determine if the patient has a significant or amblyogenic refractive error (Table 2). In younger children, ages four and younger, subjective refraction is not possible, so retinoscopy results are used for prescribing glasses. Children have a very active accommodative system, which can make determining refractive error challenging. During dry retinoscopy, using videos at distance will help to control accommodation.
Once you have obtained a solid retinoscopy, trial frame the prescription and check ocular alignment and any binocular vision testing through the trial framed prescription. In very young children, it may be difficult to get a corrected visual acuity during the first visit (it’s more a bonus, if possible!), and these patients will likely have to return for a follow-up exam. A cycloplegic refraction is also essential to determine accurate refractive error, and is recommended for all new pediatric patients.1
 |
Binocular Vision Assessment
Many children with binocular vision issues will not report traditional symptoms to a practitioner during case history. More often than not, children have been used to seeing the world one way for their entire lives, and they may not know this is abnormal. For this reason, it is imperative that a binocular vision assessment is performed on all children. To maximize efficiency considering the limited attention span in pediatric patients, we want to choose binocular vision tests that will give us the most bang for our buck. At a minimum, we need to make sure we have assessed vergence ability and amplitude, oculomotor skills and accommodation amplitude, facility and posture. Although this seems like a lot of testing, with practice a good binocular vision screening can be performed very quickly.
Accommodative amplitudes give us information about our patient’s ability to stimulate accommodation. Donder’s pull away amplitude testing can be viewed as a fun game for kids. Ask the patient to tell you when they can first see the mystery letter or shape as you pull the fixation target away from the patient’s eye monocularly.
A minimum accommodative amplitude for each child can be calculated using Hofsteder’s formula, 15-0.25(age). An amplitude that is 2D below this value is considered abnormal.11 Posture of accommodation can be quickly evaluated using the Monocular Estimation Method (MEM) retinoscopy. This technique can be used even in young children who cannot read and may be unable to do other tests of accommodation. Binocular accommodative facility (BAF) using ±2.00 flippers is another great test for screening for binocular vision disorders because it probes both the vergence and accommodative systems.
 |
|
Fixation target displayed on transilluminator, which can be ideal for performing Hirschberg and pupillary testing. Click image to enlarge. |
If a patient can successfully perform BAF, they have good ability to converge, diverge, stimulate and relax accommodation. If BAF is abnormal, performing the monocular version of this test (MAF) helps to determine if your patient has an accommodative dysfunction. This test is performed monocularly, so it isolates the accommodative system. An abnormality found during amplitude, MEM or BAF testing can be further probed at a follow-up binocular vision evaluation.
Stereopsis can be administered as a preliminary test prior to refractive error assessment. If the child did not perform well on this test, or if a significant refractive error is detected on retinoscopy, repeat the test with the trial frame refraction to see if there are any improvements.
To assess binocularity, cover test and near point of convergence should be performed on all patients. Don’t forget to use your fun fixation targets to make this an engaging activity. Based on the cover test value obtained, it is worthwhile to ensure your patient has the vergence ranges needed to compensate for their phoria and meet their visual demand. For patients presenting with an eso posture, perform base-in vergence ranges, and, for exo posture patients, perform base-out vergence ranges to screen for any binocular vision issues.
Step vergence ranges using your prism bar in free space are efficient and typically work better than smooth vergence range testing in this population. Additionally, step vergence range testing allows you to make objective assessments of the patient’s break and recovery that cannot be seen in the phoropter. This allows testing even in patients that have difficulty giving a subjective response. Sheard’s criteria suggests that a patient should have double their phoric value in reserves to maintain comfortable binocularity.12 If a binocular vision issue is suspected, further testing of all distance and near vergence ranges and vergence facility is recommended at a follow-up visit.
Oculomotor skills can be grossly assessed during extraocular motility testing as a part of your preliminary workup. When eye tracking is indicated as a concern based on the case history or screening assessments, an NSUCO saccades and pursuits test can allow for a quantitative assessment. This can be performed at the initial examination or at a follow-up.
A quick assessment of accommodation, oculomotor skills and vergence is recommended at any initial evaluation. If any testing comes back abnormal, consider bringing the patient back or refer to a colleague for a more extensive binocular vision workup. Additionally, if the patient has a significant refractive error that is being corrected for the first time or a significant change in refractive error, a follow-up visit after the patient has been wearing the prescription for at least two weeks is recommended to evaluate the binocular vision system.
Takeaways
When a red flag presents itself, make sure to bring the patient back for a more extensive binocular vision examination or refer out as appropriate. It is beneficial to know the local doctors in your area to refer to. It is crucial to know local pediatric ophthalmologists to refer to for ocular diseases. If you are not in a practice setting that is able to offer vision therapy, use the “locate a doctor” feature on the website for the College of Optometrists in Vision Development to find optometrists in your area to refer to. An excellent reference book is Applied Concepts in Vision Therapy by Leonard Press.
All optometrists can examine a child efficiently with the right tools and practice. Access to vision care for young patients is important, and providers that are comfortable examining children are always in demand. Examining pediatric patients can be both rewarding and practice building.
Dr. Krueger is an assistant professor at Nova Southeastern University and serves as site coordinator for the school’s pediatric and binocular vision residency. She is also the site coordinator for the Pediatric Eye Disease Investigator Group (PEDIG). Her special interests include binocular vision, pediatrics and learning-related vision problems. She recently earned her master’s degree in special education. She is a fellow of the American Academy of Optometry and an active member of the College of Optometrists in Vision Development. Dr. Krueger is actively involved in volunteering through the Special Olympics International organization as a clinical director.
Dr. Jenewein is an associate professor at Salus University and serves as the principal site investigator for PEDIG and the coordinator for the school’s pediatric/vision therapy residency program. Her research interests include myopia control, strabismus, and amblyopia. Dr. Jenewein is a fellow of the American Academy of Optometry and a diplomate in the Binocular Vision, Perception and Pediatric Optometry Section. They have no financial disclosures.
1. AOA. Evidence-based clinical practice guideline: comprehensive pediatric eye and vision examination. Optometric Clinical Practice. 2020;2:7. 2. Teller DY, McDonald MA, Preston K, et al. Assessment of Visual acuity in infants and children; the acuity card procedure. Dev Med Child Neurol. 1986;28(6):779-89. 3. Woodhouse JM, Adoh TO, Oduwaiye KA, et al. New acuity test for toddlers. Ophthalmic Physiol Opt. 1992;12(2):249-51. 4. Vision in Preschoolers Study Group. Preschool visual acuity screening with HOTV and Lea symbols: testability and between-test agreement. Optom Vis Sci. 2004;81(9):678-83. 5. Kulp MT, Mitchell GL. Randot stereoacuity testing in young children. J Pediatr Ophthalmol Strabismus. 2005;42(6):360-4. 6. Manny RE, Martinez AT, Fern KD. Testing stereopsis in the preschool child: is it clinically useful? J Pediatr Ophthalmol Strabismus. 1991;28(4):223-31. 7. Birch E, Shimojo S, Held R. Preferential-looking assessment of fusion and stereopsis in infants aged one to six months. Invest Ophthalmol Vis Sci. 1985;26(3):366-70. 8. Schmidt PP, Maguire MG, Moore B, Cyert L; Vision in Preschoolers Study Group. Testability of preschoolers on stereotests used to screen vision disorders. Optom Vis Sci. 2003;80(11):753-7. 9. Cotter SA, Lee DY, French AL. Evaluation of a new color vision test:“color vision testing made easy. Optom Vis Sci. 1999;76(9):631-6. 10. Bakar NFA, Chen AH, Noor ARM, Goh PP. The use of COVD-QOL questionnaire in school vision screening. Iperception. 2011;2(4):310. 11. Scheiman M, WIck B. Clinical Management of Binocular Vision: Heterophoric, Accommodative and Eye Movement Disorders. Philadelphia, PA: Lippincott Williams & Wilkins; 1994. 12. Sheard C. Zones of ocular comfort. Optom Vis Sci. 1930;7(1):9-25. |
