 |
Q:
A 66-year-old male patient presented for a cataract evaluation, stating that the vision in his left eye was blurred and has been “double” for three months. He is interested in a multifocal lens. How should I proceed?
A:
“Double vision is always a troubling complaint,” says Paul C. Ajamian, OD, center director of Omni Eye Services of Atlanta and editor of this column. Before you panic, have the patient close one eye and see if the diplopia is still present. In this case, the patient described a ghosting of letters above the actual print or signs, only from the left eye. Once we determined that, it was time to find the cause.
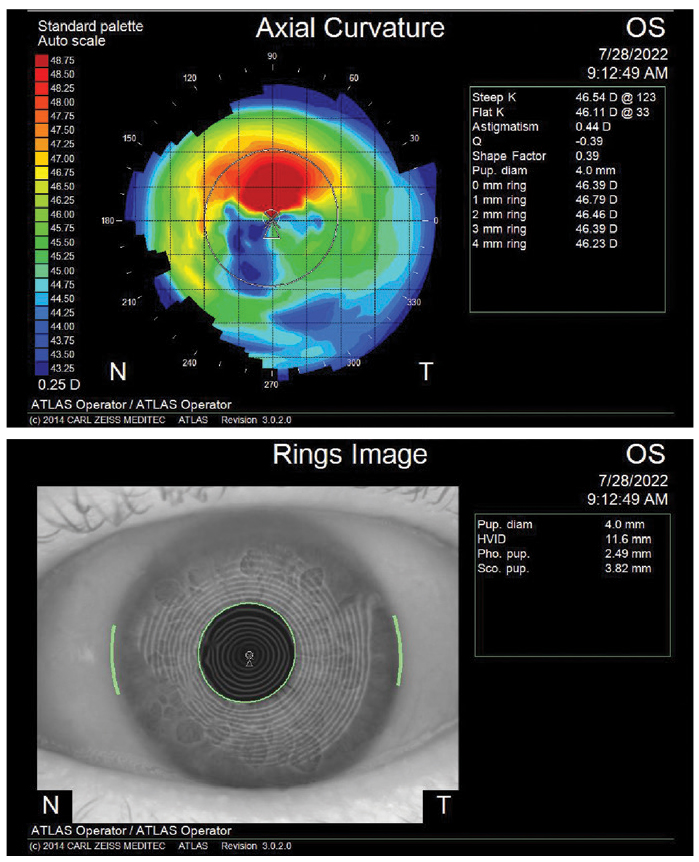
“Everything starts with corneal topography,” says Dr. Ajamian. “It is very difficult to make a proper cataract referral without it.” Look at the numbers, color map and keratoscopic rings for any irregularities. In the case of our patient, the topography in that left eye was very irregular, and caused us to take another look at the cornea.
 |
|
Fig. 1. Check the cornea for any irregularities before moving forward with cataract patients. Click image to enlarge. |
The Hard Way
The best way to prove that a subtle irregularity of the cornea is the culprit in a case such as this is with a diagnostic hard lens. Dust off your hard lens trial kit and, with a drop of proparacaine, fit the patient with an appropriate base curve lens and do an overrefraction. The results can be very revealing. In the case of our patient, the monocular ghosting totally disappeared with the lens in place, and the vision improved by several lines.
“I have seen this hard lens trick save patients from further testing and time-consuming referrals for unexplained vision loss,” Dr. Ajamian notes. Otherwise, look for other causes such as milky nuclear sclerosis, a subtle epiretinal membrane or perhaps a neurological issue that needs to be investigated with visual fields and radiologic imaging.
A Closer Look
If you didn’t see anything on the slit lamp exam the first time around, look again. The topographic map of our patient showed a steep irregular area superiorly (Figure 1). This corresponded to a subtle horizontal band of epithelial basement membrane dystrophy with maps and fingerprints above the visual axis. Before you send anyone for cataract surgery, be sure to address the lids and ocular surface. “The more pristine the ocular surface, the better the results of standard or premium lens cataract surgery,” Dr. Ajamian notes.
Convey your findings and pre-op plan to the surgeon by writing a letter that clearly outlines the patient’s goals as well as your recommendations for type of lens implant, target refraction and/or monovision. The more options discussed ahead of time, the easier the patient can make an informed decision when they see the surgeon.
No one knows your patient better than you, so share your knowledge of your patients with other providers to ensure desired outcomes.
The Plan, Stan
Our patient was a bit surprised when the talk turned from cataract removal to corneal rehabilitation. A patient with advanced map-dot-fingerprint epithelial dystrophy will not do well after cataract surgery unless the cornea is addressed first. A superficial keratectomy was recommended prior to surgery. This procedure removes the corneal epithelium down to Bowman’s membrane, particularly the area of central reduplicated epithelial basement membrane that is causing the irregular astigmatism.
After the procedure, a bandage lens is put on the eye and the patient followed over a few weeks. Several months later, assuming good healing and stable topography readings, the cataract scans can be redone and cataract surgery can be scheduled. However, proceed with caution on a multifocal IOL despite a “new” corneal surface. “A monofocal lens with reading glasses is probably still the safest bet in a case like this,” Dr. Ajamian says.
Dr. Ajamian is board certified by the American Board of Optometry and serves as Center Director of Omni Eye Services of Atlanta. He is vice president of the Georgia State Board of Optometry and general CE chairman of SECO International. He has no financial interests to disclose.
