 |
A 71-year-old man presented urgently with a bloody left eye that had been injured that morning. He had been pruning an areca palm tree when he bent down and caught the sharp end of a new shoot on his left eye. He immediately knew that it had done damage, especially when his eye started bleeding. He initially went to an Urgent Care walk-in clinic, where the physician there directed him immediately to see an eye care practitioner instead.
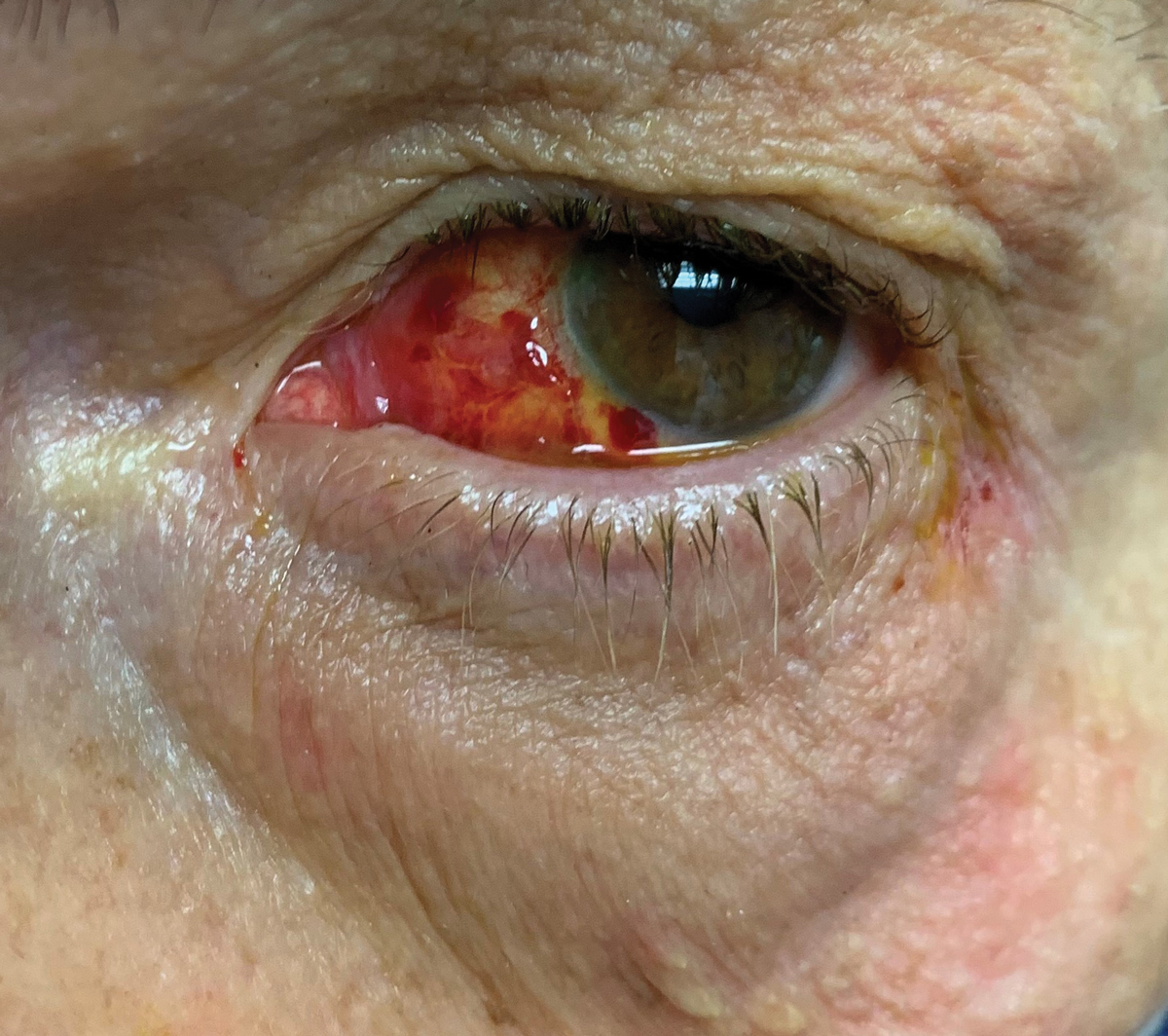
When he arrived, he reported significant ocular pain OS with tearing but no photophobia. His uncorrected visual acuity (VA) was 20/40 OD and 20/25 OS. His pupils were normal without afferent defect. Biomicroscopy revealed a corneal laceration with bare sclera visible. There were numerous dirt specs and dried blood within the wound area. There was also a mild hemorrhagic oozing in the wound. There appeared to be no breach of the sclera. The anterior chamber was fully formed and deep with no cells or flare. Intraocular pressure was 17mm Hg OS.
A dilated fundus examination showed no abnormalities and/or evidence of globe rupture or perforation. While potentially ominous due to the type of trauma that could have easily perforated the globe, the patient was fortunate in that he escaped with only a conjunctival laceration.
 |
| Mild hemorrhagic oozing in the laceration wound. Click image to enlarge. |
Wear and Tear
Conjunctival lacerations result from mechanical tearing of the tissue.1-3 Patients report a history of ocular injury from a sporting accident, assault, fall, poke, child-or-pet scratch or self-induced trauma such as eye rubbing or contact lens removal. Symptoms include variable levels of blepharospasm and discomfort, foreign body sensation, tearing and possibly photophobia if there is substantial ocular inflammation.4 Signs include sectoral conjunctival injection, subconjunctival hemorrhage and a visible conjunctival defect with retracted conjunctival edges and bare sclera.
The palpebral portion of the conjunctiva is tightly adherent to the eyelid, while the bulbar portion is loosely adherent, giving the globe mobility. The conjunctiva is reflected upon itself so that it can stretch with ocular excursion. The conjunctiva is composed of nonkeratinized, stratified, squamous epithelium overlying stromal tissue. Because the conjunctiva is far less innervated than the cornea, conjunctival injuries are less symptomatic than corneal abrasions of the same severity. Given its position, the bulbar conjunctiva has the greatest chance of sustaining injury.4
In conjunctival laceration, the tissue is torn and split, revealing bare sclera beneath. In these cases, the trauma itself acts as an antigen and sets off an inflammatory cascade resulting in vasodilation and edema of the involved and surrounding tissues.4 If the injury is more substantial, the sclera may be breeched, and dark uveal tissue may extrude through. This takes the issue in a different, more severe direction.
Treatment for conjunctival laceration begins with history, looking for possible indication of globe perforation. Assess VA initially. If discomfort and blepharospasm is intense, administer a drop of topical anesthetic. The examination should proceed in a logical fashion from external adnexa to dilated fundus examination.
Evert the eyelids and scrutinize the fornicies for foreign material. Instill fluorescein dye (preferably without anesthetic) to assist in identifying defects. The lesion should be photographed, if possible, and measured using the height and width of the biomicroscope beam.
Perform close observation of the sclera to assess for possible globe penetration, especially if the injury came from a sharp object.5,6 If particulate matter is present, clean the lesion after instilling anesthetic. Observe the anterior chamber for any evidence of inflammation. Most importantly, assess and record the depth of the anterior chamber, as flattening or shallowing indicates a globe perforation.
Use forceps or moistened cotton-tipped applicator with topical anesthesia to manipulate the ragged areas of conjunctiva back into position. Bleeding can be arrested with light, direct pressure. If possible, tonometry should be performed as hypotony also may indicate a globe perforation. Complete a dilated examination (either at time of initial evaluation or at follow-up) to rule out any posterior effects from the trauma.
 |
|
Be sure to lavage all dirt and blood with sterile saline wash. Click image to enlarge. |
Treatment
The eye can be either patched or left open. If the eye is not patched, treatment includes topical broad-spectrum antibiotic solution QID. Consider topical cycloplegia, either applied in office or prescribed QD-BID, depending upon the severity of the injury and degree of inflammatory discomfort. Additionally, prescribe a topical nonsteroidal anti-inflammatory (NSAID) QD-QID for local analgesia.
Topical antibiotic ointments can be used for increased contact time and extra comfort cushioning but are often not tolerated well as they blur vision. Topical steroids have the potential to slow healing and, in the setting of trauma, may be postponed until initial tissue healing takes place. Topical antibiotic/steroid combination drops and/or ointments are a reasonable alternative if inflammation must be addressed on the day of the injury.
Small conjunctival lacerations (<1cm) will heal within a week without special attention. Larger lacerations, after appositional placement of the tissue edges, can be remediated with antibiotic ointment and pressure patching for 24 hours. Repair with either sutures or tissue glue is only necessary for only the largest lesions (> 2cm). Bed rest, limited activity, cold compresses, artificial tear drops and over-the-counter analgesics such as acetaminophen or ibuprofen can relieve acute pain for a day or so. Acetaminophen can be recommended in cases where there is bleeding as it does not encourage antiplatelet effects.
Conjunctival lacerations without globe perforation tend to be uncomfortable and unpleasant but will resolve with only a modicum of care and triage.
Laceration Care
For the patient presented here, he was carefully assessed for a globe perforation due to the nature of his injury. Following topical anesthesia, the conjunctival edges were manipulated to fully assess the underlying sclera, which was intact. His IOP was measured, and anterior chamber was assessed to eliminate the possibility of hypotony and shallowing, both of which would indicate a globe perforation. A dilated exam was also performed to rule out tears, detachments and other untoward traumatic effects.
After this assessment was performed, all dirt and blood were lavaged out with sterile saline wash. The edges of the abrasion were manipulated together with a cotton-tipped applicator. He was prescribed topical bacitracin-polymyxin B ointment QID. He was not patched or cyclopleged. Acetaminophen was recommended for pain. A 24-hour follow-up telephone call revealed that he felt much better and that the acetaminophen helped sufficiently.
When he returned for follow-up one week later, the conjunctival laceration was well healed with mild residual subconjunctival hemorrhage. He was instructed to stop all medications and to wear eye protection when gardening as the next time he might not be as fortunate with a similar injury.
Takeaways
Conjunctival lacerations are minor problems that typically resolve with minimal intervention, yet patients often present with great anxiety. Hemorrhaging causes great concern, even though there may be little pain or other symptoms. While it is important to rule out a penetrating injury, you can safely reassure most patients that they have a simple “cut” on their eye and that it will heal in a few days.
Dr. Sowka is an attending optometric physician at Center for Sight in Sarasota, FL, where he focuses on glaucoma management and neuro-ophthalmic disease. He is a consultant and advisory board member for Carl Zeiss Meditec and Bausch Health.
1. Gordon KD. The incidence of eye injuries in Canada. Can J Ophthalmol. 2012;47(4):351-3. 2. Leinert J, Griffin R, Blackburn J, McGwin G Jr. The epidemiology of lawn trimmer injuries in the United States: 2000-2009. J Safety Res. 2012;43(2):137-9. 3. Locke LC. Conjunctival abrasions and lacerations. J Am Optom Assoc. 1987;58(6):488-93. 4. Murthy SI, Das S, Deshpande P, et al. Differential diagnosis of acute ocular pain: teleophthalmology during COVID-19 pandemic—a perspective. Indian J Ophthalmol. 2020; 68(7): 1371-9. 5. Freidman NJ, Kaiser PK. The conjunctiva. In: Freidman NJ, Kaiser PK. Essentials of Ophthalmology. Philadelphia, PA, Saunders Inc; 2007:149-59. 6. Muller L, Kohnen T. Scleral and corneal laceration with iris prolapse caused by an eagle claw. Graefes Arch Clin Exp Ophthalmol. 2005;243(4):377-9. |
