 |
|
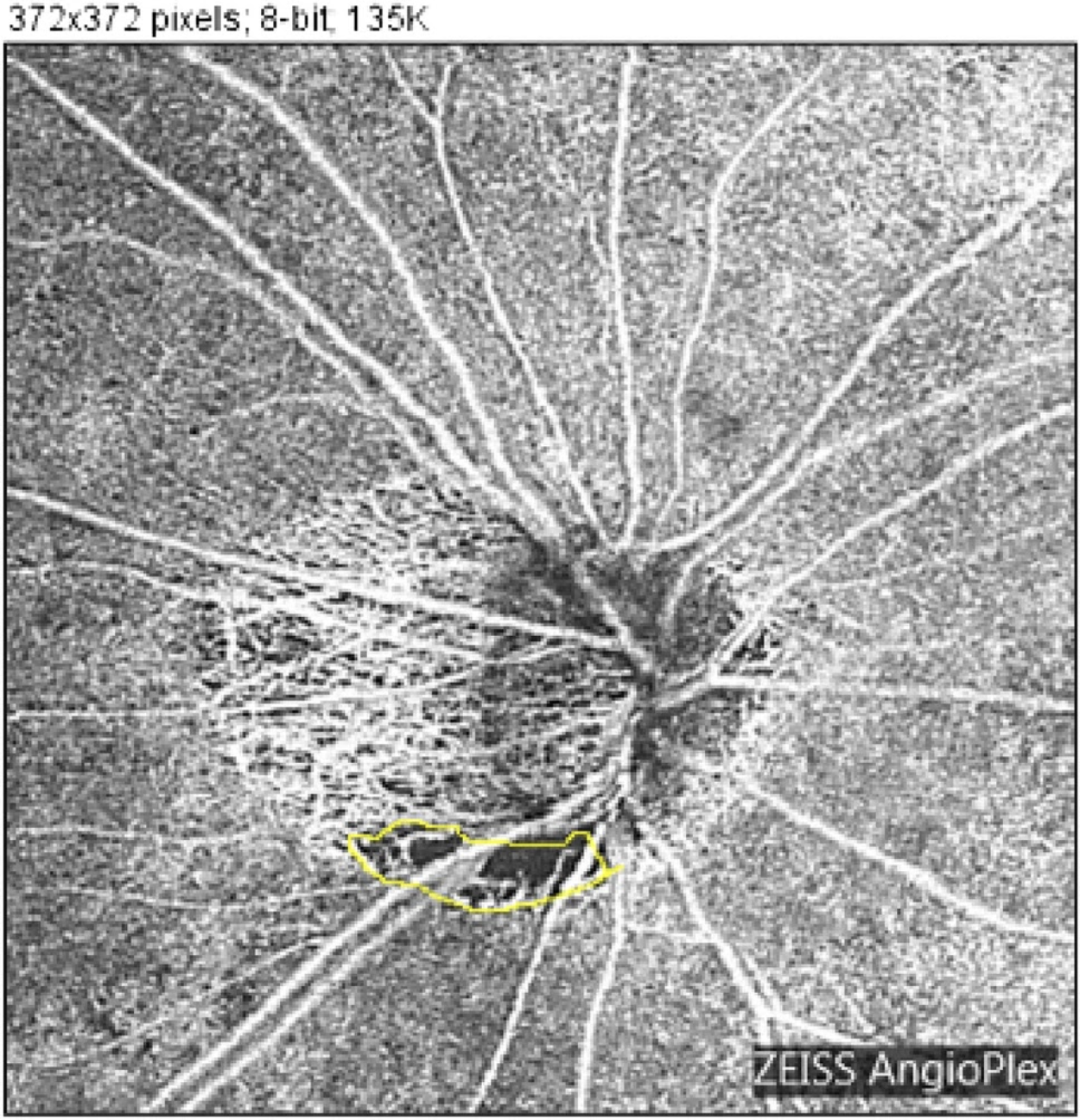
A higher proportion of eyes in the high myopia group transitioned from not showing microvasculature dropout at baseline to developing it throughout the follow-up. Photo: Igarashi R, et al. Sci Rep. 2023;13;20601. Click image to enlarge. |
Detecting and monitoring glaucoma in highly myopic eyes can be diagnostically difficult due to morphologic changes in the optic nerve head (ONH) and parapapillary region. Optical coherence tomography angiography (OCT-A) has enabled the evaluation of localized perfusion defects known as choriocapillaris microvasculature dropout. These defects are of particular interest as they occur in the parapapillary choroid, which is supplied by the short posterior ciliary arteries, the same vessels that supply the lamina cribrosa of the ONH. Nevertheless, the association between the rates of choroidal microvasculature dropout change and the rates of change in ganglion cell layer thickness in glaucoma eyes with myopia has not yet been reported. A recent study published in American Journal of Ophthalmology determined that microvasculature dropout area and angular circumference changes over time were significantly, albeit modestly, associated with faster ganglion cell inner plexiform layer (GCIPL) thinning in myopic POAG eyes over a mean follow-up of 4.4 years.
The cohort study organized 238 eyes from 155 POAG and glaucoma suspect patients into no-myopia (axial length (AL) ≤ 24mm; n=78 eyes), mild myopia (24mm< AL ≤ 26mm; n=114 eyes), and high myopia (AL > 26mm; n=46 eyes). Eyes with a minimum of three visits and 1.5 years of follow-up with both OCT-A and OCT macula scans were included. Presence, area and angular circumference of juxtapapillary microvasculature dropout were evaluated on en face choroidal images and horizontal B-scans obtained from OCT-A imaging.
Juxtapapillary choriocapillaris microvasculature dropout was detectable in over 70% of POAG eyes across all groups, including those with high myopia. Notably, a higher proportion of eyes in the high myopia group transitioned from not showing microvasculature dropout at baseline to developing it throughout the follow-up.
The mean microvasculature dropout area rates of change were largest in the high and mild myopia groups (0.04mm2/year in both groups), followed by the no-myopia group (0.03mm2/year). The mean microvasculature dropout angular circumference rates of change were highest in the mild myopia group (8.7º/year), followed by the high myopia and no-myopia groups (8.1º/year, and 7.4º/year, respectively).
While the mean global GCIPL thinning rates between eyes with microvasculature dropout at baseline compared with eyes without were similar in all myopia groups, the rates of microvasculature dropout area change were significantly faster in all myopia groups with baseline microvasculature dropout. Multivariable models revealed that the rates of GCIPL thinning over time were significantly associated with rates of microvasculature dropout angular circumference change and microvasculature dropout area change.
“Although the precise mechanism underlying the relationship between microvasculature dropout and GCIPL loss in glaucomatous eyes remains uncertain, several hypotheses have been proposed to elucidate this relationship,” the study authors wrote in their paper. “One possible hypothesis is that the development of microvasculature may be associated with a thinner choroid in the parapapillary region of glaucomatous eyes and thereby reducing blood flow to the ONH.”
Using OCT-A to detect microvasculature dropout may provide an additional tool for monitoring macular structural changes in this cohort of eyes.
Jiravarnsirikui A, Belghith A, Rezapour J, et al. Rates of choriocapillaris microvascular dropout and macular structural changes in glaucomatous optic neuropathy with and without myopia. Am J Ophthalmol. July 7, 2024. [Epub ahead of print]. |