Findings from a recently published study highlight the advantages of en face OCT imaging to identify complete RPE and outer retinal atrophy (cRORA) lesions as well as the importance of obtaining dense raster B-scans alongside the grading of adjacent B-scans when identifying incomplete retinal pigment epithelium and outer retinal atrophy (iRORA), particularly in non-horizontal dimensions.
Data from this analysis, which appears in American Journal of Ophthalmology, also showed that, 27.5% of iRORA lesions were part of larger cRORA lesions when evaluated with the en face method.
In this comparative diagnostic analysis of prospective study data, patients with late, non-exudative AMD underwent same day 6x6 mm macular scans using both spectral-domain OCT (SD-OCT) and swept-source OCT angiography (SS-OCT-A). Researchers generated SS-OCT-A and SD-OCT en face images from a sub-RPE slab positioned 64-400μm below Bruch's membrane.
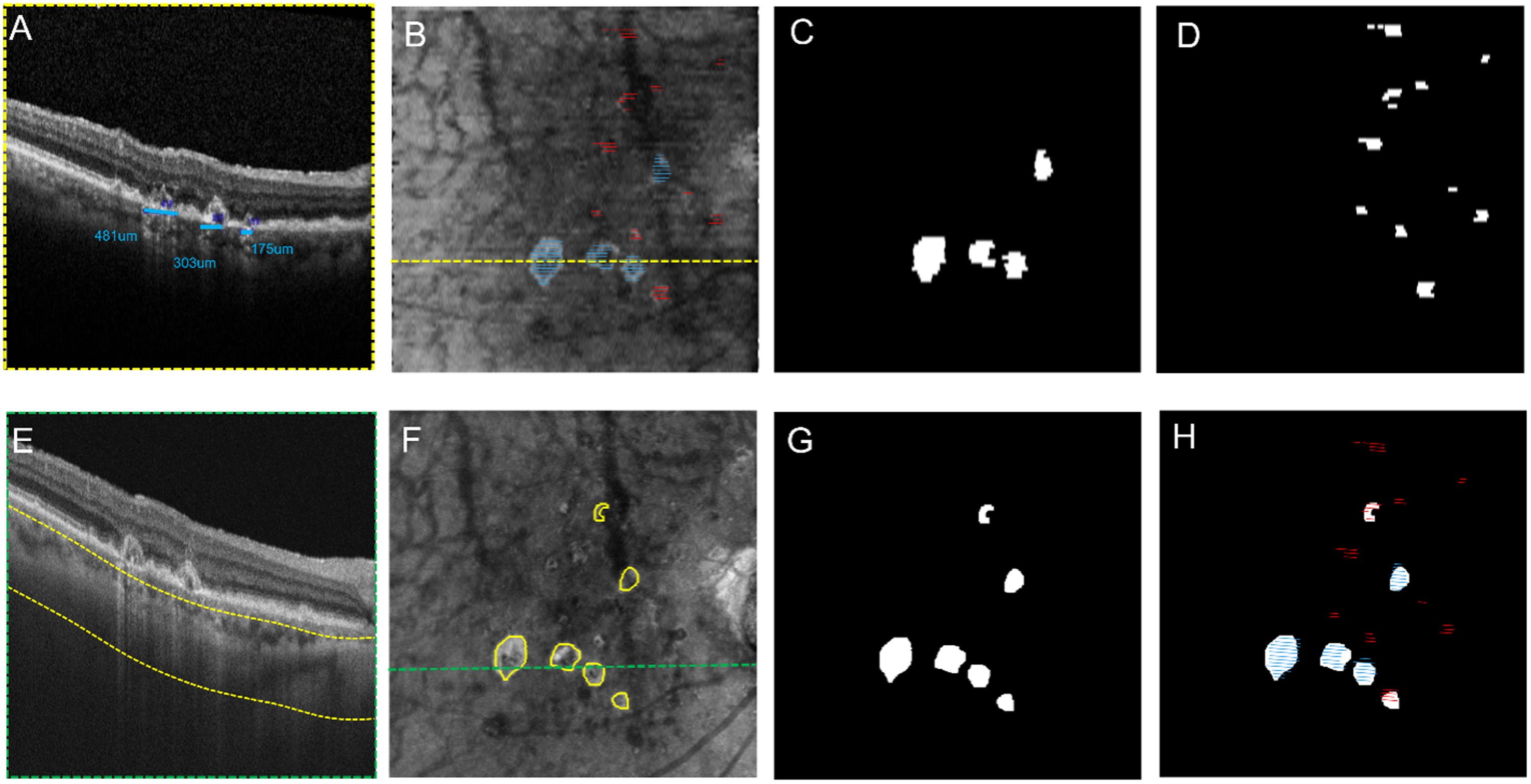 |
| A recent study demonstrates that en face OCT imaging effectively identifies complete RPE and outer retinal atrophy (CRORA) lesions, while also emphasizing the necessity of dense raster B-scans and adjacent B-scan grading for accurate detection of incomplete (iRORA) lesions, especially in non-horizontal dimensions. These images from the study show the process of identification of iRORA and cRORA in a representative eye using SD-OCT and SS-OCT instruments: (A) SD-OCT B-scan with blue lines denoting cRORA, (B) En face image of sub-RPE slab obtained from the SD-OCT scan. Persistent choroidal hypertransmission defects (hyperTDs) are visible across the entire scan area with the overlay of lines corresponding to cRORA (blue lines) and iRORA (red lines). (C) An en face cRORA mask was generated based on B-scan gradings on SD-OCT. (D) An en face iRORA mask was generated based on its B-scan gradings on SD-OCT. Photo: Cheng Y, et al. Am J Ophthalmol. October 8, 2024. Click image to enlarge. |
In this comparative diagnostic analysis of prospective study data, patients with late, non-exudative AMD underwent same day 6x6 mm macular scans using both spectral-domain OCT (SD-OCT) and swept-source OCT angiography (SS-OCT-A). Researchers generated SS-OCT-A and SD-OCT en face images from a sub-RPE slab positioned 64-400μm below Bruch's membrane.
Data revealed a high degree of agreement (99.6%) between the gradings of complete retinal pigment epithelium and outer retinal atrophy lesions and persistent hypertransmission defects (hyperTDs), according to the study authors. However, they noted, 27.4% of incomplete retinal pigment epithelium and outer retinal atrophy lesions were contained within persistent hyperTDs.
“This discrepancy was due to the finding that 27.5% of iRORA lesions were diagnosed as having a greatest linear horizontal dimension of < 250 μm on B-scans, but on en face images, these B-scan defined iRORA lesions were found to have a greatest linear dimensions in the non-horizontal dimension that were ≥ 250 μm,” the investigators explained in their recent paper.
While discussing their research in AJO the study authors noted that this analysis underscores the vital need to carefully assess choroidal hypertransmission defects across all neighboring B-scans when classifying iRORA lesions with a dense OCT B-scan imaging pattern to identify instances where iRORA lesions are actually cRORA lesions. In contrast, en face OCT imaging effectively reveals persistent hyperTDs, which are equivalent to cRORA lesions.
“To ensure accurate differentiation between iRORA and cRORA when grading B-scans, it is essential to examine adjacent B-scans for a comprehensive understanding of the extent of choroidal hyperTDs and the accompanying changes in the RPE and outer retina,” they concluded. “Most notably, detection of persistent hyperTDs on en face images is much easier than scrolling through 97 or more B-scans to identify these lesions. Additionally, the use of automated algorithms to identify persistent hyperTDs improves the efficiency of lesion detection, streamlining the diagnostic process.”
| Click here for journal source. |
Cheng Y, Fleckenstein M, Schmitz-Valckenberg MS, et al. Comparison between OCT B-scan and en face imaging for the diagnosis of early macular atrophy in age-related macular degeneration. Am J Ophthalmol. October 8, 2024 [Epub ahead of print]. |