 |
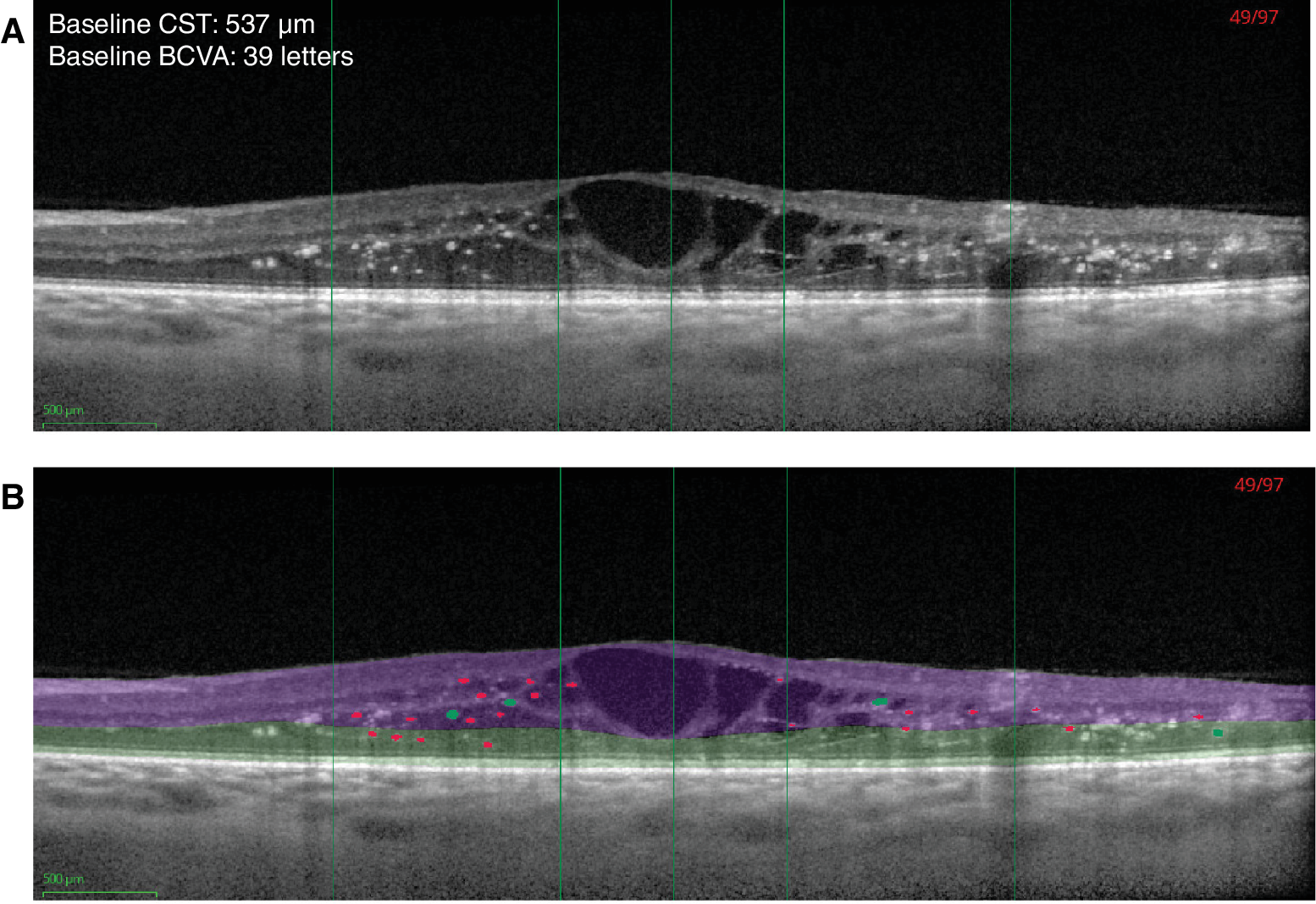
| This image from the study shows automated hyperreflective foci (HRF) segmentation on SD-OCT without (A) and with (B) segmentation of layers. HRF ≤50µm are shown in red and larger (>50µm and ≤100µm) intraretinal hyperreflective objects in green. The algorithm filtered out objects >100µm; hence, these objects are not colored in the figure. ETDRS rings are indicated with green vertical lines (center, 1mm and 3mm diameter rings). Inner retina is shown in purple and outer retina in green. Photo: Von Schulthess EL, et al. Invest Ophthalmol Vis Sci. 2024;65(5):26. Click image to enlarge. |
In diabetic macular edema (DME), hyper-reflective foci (HRF) has been linked to disease severity and progression. So, in a new study, researchers assessed whether HRF co-localize with cystoid intraretinal fluid (IRF) in patients with DME. They found that HRF was present in most DME patients and may be linked to disease severity.
A total of 1,527 baseline (SD-OCT volume scans from Phase III clinical trials were segmented using a deep-learning-based algorithm to detect hyper-reflective foci, in which the HRF count and volume were assessed. HRF distributions were analyzed in relation to best-corrected visual acuity (BCVA), central subfield thickness and IRF volume, and Diabetic Retinopathy Severity Scores in groups. Co-localization of HRF with IRF was calculated in the central 3mm diameter using the en face projection.
HRF was present in virtually all DME patients (up to 99.7%). This is similar to previous reports on the prevalence of HRF, where approximately 90% of eyes with DME were shown to exhibit this on SD-OCT.
“Although the quantity of HRF in the inner versus outer retina was comparable in the 3mm diameter, twice as many HRF were present in the inner retina of the central subfield compared with the outer retina,” the researchers noted in their paper for Investigative Ophthalmology & Visual Science. “This imbalanced distribution may suggest a greater rate of HRF removal in the outer retina of the central subfield, or may be due to the topography of Henle’s fiber layer in the central subfield.”
They observed higher HRF volumes with increasing Diabetic Retinopathy Severity Scores, greater central subfield thickness and the presence of cystoid IRF. “Furthermore, we noted a trend for worse BCVA with greater HRF volumes,” the authors noted. “These findings suggest that HRF are markers for disease severity. However, the median HRF volume, as well as the median CST, was slightly lower in eyes with PDR than with severe NPDR.” This, they speculate, may be due to one third of study eyes in the proliferative diabetic retinopathy (PDR) group received panretinal photocoagulation (PRP) more than three months prior to study enrollment, “an intervention known to cause retinal thinning and result in reduced severity of retinopathy.” Consequently, the authors added, prior PRP may have confounded the relationship between DR severity and HRF in study eyes with PDR.
In addition to the above-mentioned potential relationship between cystoid IRF and HRF volumes, the shape distribution of HRF in the en face SD-OCT volumes followed the distribution of cystoid IRF, which is in line a previous study that showed co-localization with intraretinal hyper-reflective material, in particular hyper-reflective fluid.
“We recognize that the correlation between HRF distribution and IRF localization is modest; however, given that the shape distribution of the former follows that of the latter, we therefore believe that these OCT features are linked and hypothesize that the HRF in DME may originate within IRF cysts,” the authors concluded in their IOVS paper. “For future studies, we recommend the use of automated approaches to analyze full SD-OCT volume scans to minimize bias. Whereas volumetric analyses constitute the most robust approach, incorporating size differences into the measure, similar results can also be obtained with the more tangible measure of HRF counts, providing the number of B-scans is consistent throughout the study population. Because the link with measures of disease severity is greater in the 3mm diameter ETDRS ring, this may be the more relevant area of assessment.”
Von Schulthess EL, Mauntz A, Chakravarthy U, et al. Intraretinal hyper-reflective foci are almost universally present and co-localize with intraretinal fluid in diabetic macular edema. Invest Ophthalmol Vis Sci. 2024;65(5):26. |