Ease the Burden of GlaucomaThe July 2023 issue of Review of Optometry centers around one of the toughest diseases to diagnose and monitor: glaucoma. The 29th annual glaucoma report targets dozens of areas where some ODs struggle to move beyond the fundamentals. Check out the other articles featured in this issue:
|
Think about this patient scenario, which you’ve likely encountered before: You enter the exam room to assess a middle-aged, hyperopic female. While performing biomicroscopy, you notice that she has a narrow van Herick angle and an elevated intraocular pressure (IOP).
These types of cases present a clinical dilemma in which four critical questions must be answered:
1. Should we dilate?
2. Should we perform gonioscopy?
3. Should we perform or recommend a laser peripheral iridotomy (LPI)?
4. Should we refer for cataract surgery?
This article will attempt to answer these questions using two patient case examples and the findings of various clinical trials with the aim of clarifying some nuances of dealing with patients across the narrow-angle spectrum.
Case One: Patient with previously diagnosed narrow angles presents for exam 18 months after missing follow-up
A 60-year-old Hispanic male presented for an exam. He was previously diagnosed with anatomic narrow angles and instructed to return in six months for continued angle assessment. Unfortunately, he canceled that appointment and did not return until two years later, when he reported mild changes in his distance and near vision. His refraction was +2.00 -1.00x010 OD and +2.00 -0.75x125 OS, both correctable to 20/20 and both glare testing to 20/40. Corneal-corrected IOP (ccIOP) by Ocular Response Analyzer was 13.5mm Hg OD and 13.2mm Hg OS.
Should we dilate this patient? To help make this determination, we can look at the findings of the Zhongshan Angle-Closure Prevention (ZAP) study, where primary angle-closure suspects (PACS) were dilated with 1% tropicamide and 2.5% phenylephrine six to seven times throughout follow-up. The results showed that the risk of an angle-closure attack was uncommon (one in 1,587 dilations).1 The study authors were concerned enough about potentially creating angle closure that they treated every patient with 250mg acetazolamide. For patients who had a post-dilation IOP increase of 8mm Hg or more, topical brimonidine and pilocarpine were also used. This may have altered the natural course of angle-closure disease resulting in underestimation.
It is worth noting that all the patients who closed in the ZAP study had all four quadrants closed at baseline and an average of +4D of hyperopia, while the mean was +2D. The Northern Ireland Diabetic Retinopathy Screening Program dilated all patients regardless of risk factors and found an incidence of angle closure of one in 31,755 patients.2
It is difficult to determine the appropriateness of dilation without first performing gonioscopy, which leads us to the next question:
Should we perform gonioscopy? This test should always be performed prior to dilation when narrow angles are suspected. A gonioscopy lens should be as ubiquitous as a 90D or 20D lens in optometric exam rooms. In our patient, gonioscopy showed posterior trabecular meshwork (TM) as the last structure seen, and there was greater than 180° of iridotrabecular contact. The amount of iridotrabecular contact was estimated to be around 270°. Anterior segment optical coherence tomography (AS-OCT) showed a narrow angle (Figure 1A). We also performed indentation gonioscopy, which involves applying pressure to the cornea using a small-footprint gonio lens to determine if peripheral anterior synechiae (PAS) exist, which they did not.
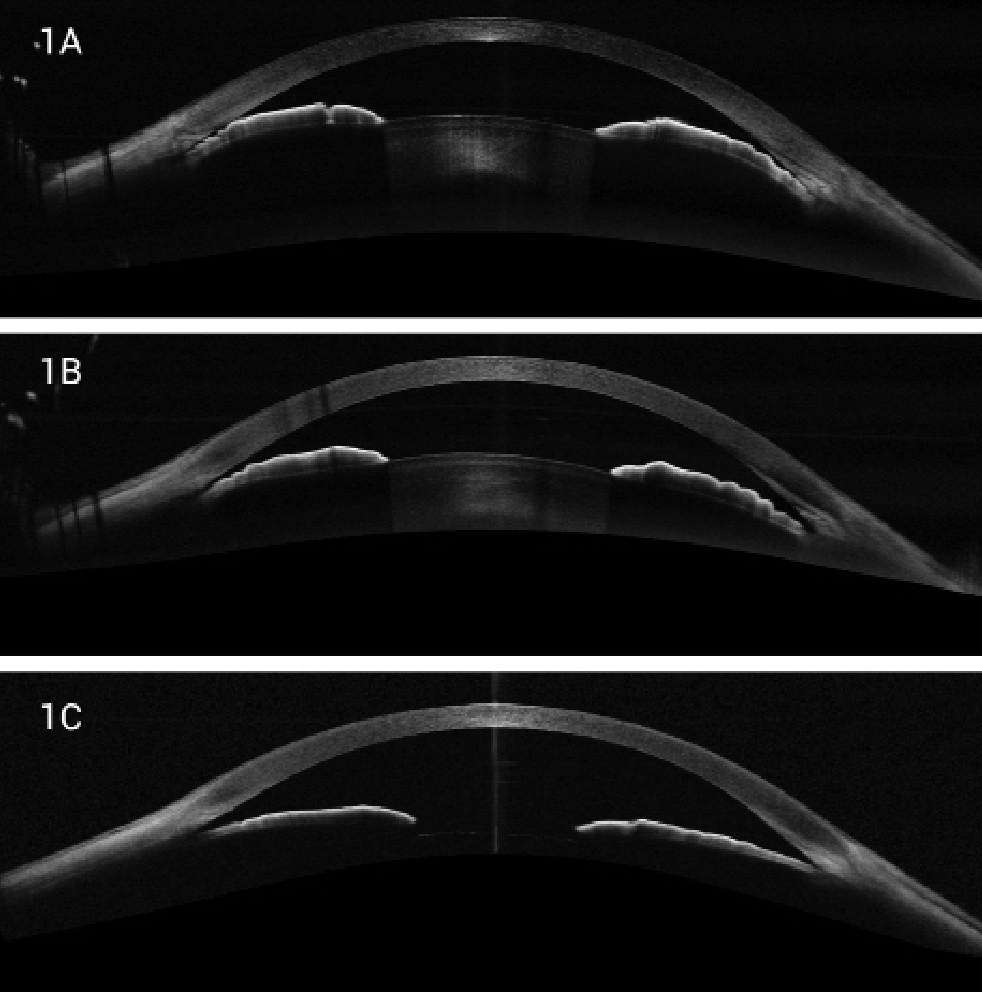 |
| Fig. 1. (A) Edge-to-edge OCT image of narrow angle with iridotrabecular contact. (B) OCT image of same eye after LPI. Note the angle slightly more open. (C) OCT of same image after cataract extraction. Note the flattened iris position with significant angle opening. Click image to enlarge. |
In our patient, even though the angle was quite narrow by gonioscopy and AS-OCT, we felt justified in dilating due to the need for a proper nerve and nerve fiber layer assessment. Clinicians should consider performing a post-dilation IOP measurement with special attention if the IOP increases 8mm Hg or more. It may also be reasonable to treat with 250mg acetazolamide, brimonidine and pilocarpine as in the ZAP protocol.
We proceeded to dilate with 0.5% tropicamide and rechecked his IOPs by Goldmann applanation tonometry post-dilation, which measured 18mm Hg OD and 19mm Hg OS. His cup-to-disc ratios were graded at 0.4x0.4 OD and OS and his lenses were nuclear sclerosis grade 1. Visual fields and OCT were unremarkable with no evidence of glaucomatous conversion, leading to the diagnosis of PACS.
Based on findings of the ZAP study, we generally dilate all but the highest-risk individuals, including those with 360° iridotrabecular contact, extensive PAS, shallow anterior chamber depth and/or greater than +3D hyperopia. If the need is great that day, we will dilate even the high-risk patients but make sure to perform post-dilation tonometry. We also carefully discuss angle-closure symptoms as well as inform them about our 24-hour on-call service. If we determine that the patient will need frequent dilations in the future, we recommend LPI.
Should we perform or recommend LPI? Ever since the 1993 landmark study by Wilensky found that 6% of angle-closure suspects developed angle closure over a mean of 2.7 years, optometrists and ophthalmologists have viewed narrow angles as a problem best managed prophylactically with LPI.3 However, recently released long-term data from the ZAP study presents evidence to suggest that LPI may be warranted specifically in patients at highest risk of conversion from PACS to primary angle closure (PAC).
The ZAP study—the largest single-center clinical trial for patients at risk of PAC—enrolled 889 patients and randomly treated one eye with LPI while the other acted as a control. The 14-year data showed that while eyes treated with LPI showed a 69% reduced risk of PAC occurrence, even after 14 years, the cumulative risk of progression to PAC was quite low.1
In the ZAP study cohort, the number needed to treat to stop one case of PACS from converting to PAC was 44 at year six and 12.35 at year 14. The number of patients needed to treat to prevent one case of PAC glaucoma (PACG) was 126 at year six. There were 6.3 acute PACs per 10,000 dilations. The study authors concluded, “prophylactic LPI should be recommended preferentially to those at the highest risk (higher IOP at baseline, shallower limbal anterior chamber depth and central anterior chamber depth) of angle closure because the annual incidence of PAC was low.”1
A second study that examined the treatment efficacy of LPI in PACS was the Singapore Asymptomatic Narrow Angles Laser Iridotomy Study (ANA-LIS), which enrolled 480 patients. Similar to ZAP, ANA-LIS randomly treated one eye with LPI with the other being a control.4 Results showed that PACS eyes with LPI had a 45% reduced risk of converting to PAC. The number needed to treat to prevent one case of PACS from becoming PAC was 22 at five years and 103.1 for PACG.1 The authors also concluded that the overall incidence of PAC or PACG in PACS is low (10.21% over five years).
Both the ZAP and ANA-LIS studies focused on patients of Chinese ethnicity that typically have higher rates of angle closure than those from the United States. As it relates to the US, Yoo et al. presented a large retrospective case study to analyze the rate of conversion from anatomical narrow angle/PACS to PACG. The study analyzed conversion over a six-year period. The overall conversion rate as indicated by practitioners per ICD-10 code was 4.13% per year.5 They found that likelihood of conversion particularly increased among the elderly.
Because the level of iridotrabecular contact in this patient was well over 180° and the angle OCT was ominous, we scheduled him for LPI within a week. LPI had a positive effect on the angle opening, but less than expected (Figure 1B). We concluded that the mechanism was primarily phacomorphic.
While we approach each PACS patient individually, in our clinics we generally recommend LPI if the patient mentions symptoms of angle closure, has a family history of angle-closure disease, has at least +3.00D of hyperopia or needs frequent dilation. Family history is arguably even more important in angle-closure disease than in POAG, with standardized incidence rations being three times higher in angle-closure cases.6 For the record, the patient in case one reported no family history of glaucoma or angle closure.
Should we proceed with cataract surgery? While LPI opened the angle slightly in the patient from case one, we decided to continue with careful monitoring. At the four-month post-LPI visit, the angle and IOP was unchanged, but the patient complained of increasing night glare, and we proceeded with cataract surgery. This flattened the iris configuration and opened the angle further (Figure 1C). We now monitor this patient yearly.
 |
|
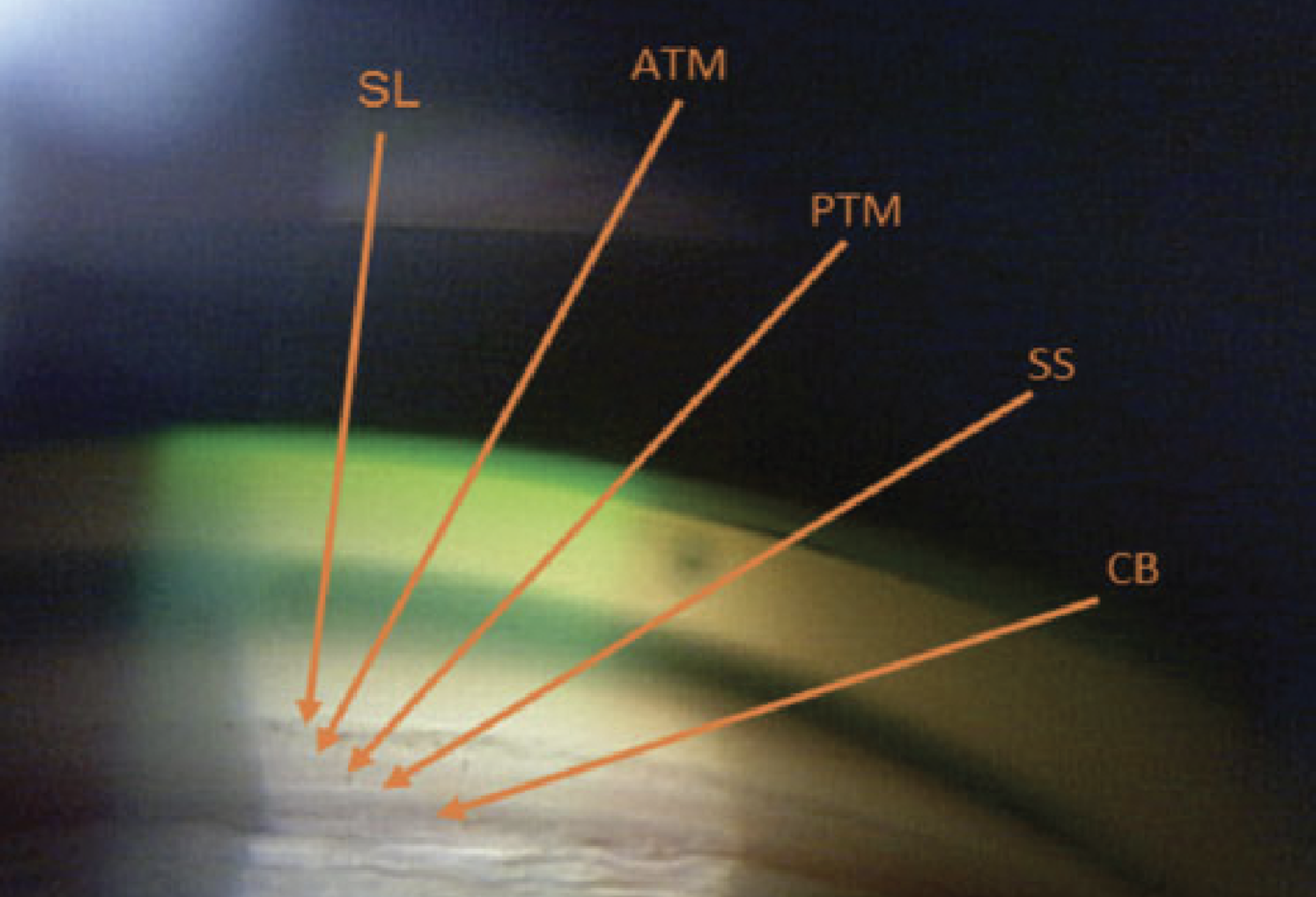
Fig. 2. The ciliary body is the most posterior structure visible, followed by the scleral spur, posterior TM, anterior TM and, finally, Schwalbe’s line. Click image to enlarge. |
General Assessment Basics
It’s important to first understand how we classify open vs. narrow angles so we can become better diagnosticians behind the gonioscopy lens. A “narrow angle” is that in which there is greater than 180° of iridocorneal contact. There are three angle closure subtypes: PACS, PAC and PACG.7-8
A PACS is defined as a subject with narrow angles (<180° of TM seen clinically) and the absence of PAS.9-10 In PACS, IOP remains normotensive (<21mm Hg) without the presence of optic atrophy or visual field deficits.11
In PAC, there is appositional occlusion of the TM and peripheral iris.12-13 The primary underlying mechanism in PAC is pupillary block. Pupillary block initially begins with increased interaction between the iris and anterior lens. As aqueous fluid attempts to flow anteriorly, resistance builds posteriorly resulting in an anterior bowed appearance (iris bombé). In the mid-dilated position, the flaccid peripheral iris moves laterally to connect to the TM and induce angle closure. Plateau iris is an anatomical variant in which the ciliary body is positioned more anteriorly, leading to mechanical contact with the TM.14 Plateau iris is a leading cause of PAC in younger individuals.
Angle closure is rare in anterior chamber depths exceeding 2.5mm.12 The average anterior chamber depth of eyes with PAC is approximately 1.8mm. This is 1mm shorter than normal eyes. Contributing factors include exaggerated lens vaulting or anterior lens positioning which accounts for approximately 0.65mm of anterior chamber depth shallowing. Increased lens thickness also plays a role, which induces roughly 0.35mm of anterior chamber depth shallowing. Average lens thickness in PAC eyes ranges from 4.24mm to 5.02mm vs. 4.04mm in non-PAC control eyes.15 PAC may be acute or chronic.
During acute angle-closure attack, patients present with an acute rise in IOP (typically >30mm Hg). They also present with several key characteristics including two of the following: ocular or periocular pain, nausea or vomiting and/or visual halos, in addition to at least three of the following: conjunctival injection, a mid-dilated pupil, microcystic corneal edema and/or a shallow anterior chamber.16
In secondary angle-closure glaucoma, various mechanisms are responsible for angle closure and result from either an anterior “pulling” of the peripheral iris into the angle to occlude the TM (e.g., neovascular membranes from ischemia, PAS secondary to inflammation, endothelial dystrophies, trauma) or a posterior “pushing” of the iris and ciliary body forward to occlude the angle (e.g., pupillary block from PAS, lens displacement, vitreous displacement inducing secondary pupillary block, space-occupying lesions of the ciliary body or posterior segment, drug-induced choroidal effusion [topiramate, sulfonamides] or secondary to glaucoma surgery and/or ciliary block).17
PACG is classified by narrow angles (as noted previously, these are defined by greater than 180° of iridocorneal contact) with chronically elevated IOP >21mm Hg and evidence of glaucomatous optic neuropathy with corresponding visual field defects.18 Comparatively, individuals with PACG tend to have more diffuse visual field defects than those with POAG, while degrees of glaucomatous optic atrophy remain the same.19 Like PAC, PACG may be acute or chronic.
PACG Prevalence
In 2020, a meta-analysis was performed including literature over the last 20 years as it related to global prevalence of PACG. It was determined that as of 2020, PACG affected approximately 17.14 million individuals older than 40 globally.20 Predictive trends were updated to suggest 20 million will be affected by 2030 and 23 million by 2040, a comparatively lower trend than suggested in a previous study.21 This may in part be due to improved methods of detection and management of PACS/PACG.
PACG Risk Factors
A patient’s risk of developing PACG can increase from various factors such as age, female sex and South Asian populations.20-21 As it relates to the pathogenesis of PACG, lenticular changes from aging contribute to crowding of the angle and pupillary block. Compared with male counterparts, female subjects presented with narrower angles and greater shallowing of the anterior chamber depth with age. Asian populations accounted for 70% of the PACG population worldwide. Several studies suggest South Asian irises are thicker and stickier, leading to PAS formation and enhanced iridocorneal contact.22
Angle Anatomy
Although underused in practice, gonioscopy remains the standard of care in angle assessment.23 The most posterior structure visualized in an open angle is the ciliary body, which is found between the iris root and scleral spur. The next structure visualized anterior to the ciliary body is the scleral spur, which is typically white or gray and serves as the anchor for the ciliary muscle. Next up is the TM, which is subdivided into the anterior (nonfunctional) and posterior and filters aqueous into Schlemm’s canal. Finally, the most anterior angle structure is Schwalbe’s line, which represents the end of a clear cornea (Figure 2, above).
Grading Systems
There are three gonioscopy grading systems that exist to better understand the anatomy of the angle: Scheie, Shaffer and Spaeth.24-25
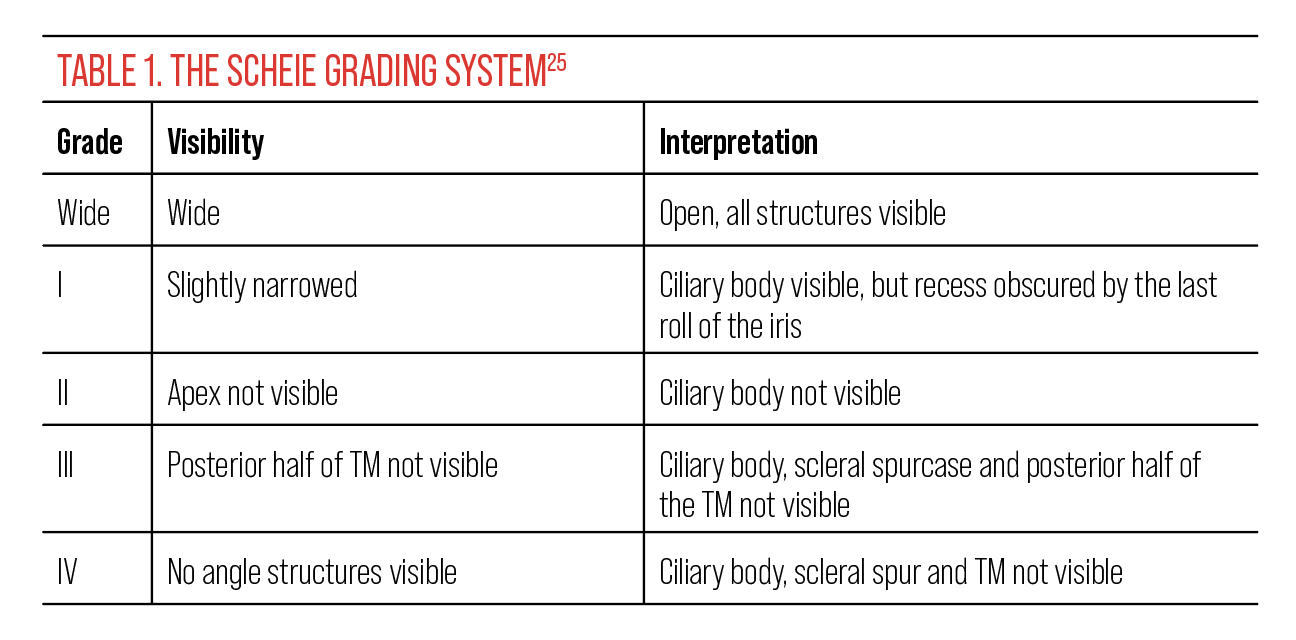 |
The Scheie classification system uses Roman numerals to describe angle depth based on visible structures in which the larger the number, the narrower the angle (Table 1).24 With this system, grade 0 indicates all structures are visible, whereas grade 4 indicates only Schwalbe’s line is visible. The Scheie grading system also provides information regarding angle pigmentation on a scale from 0 (no pigment) to IV (heavy pigment).
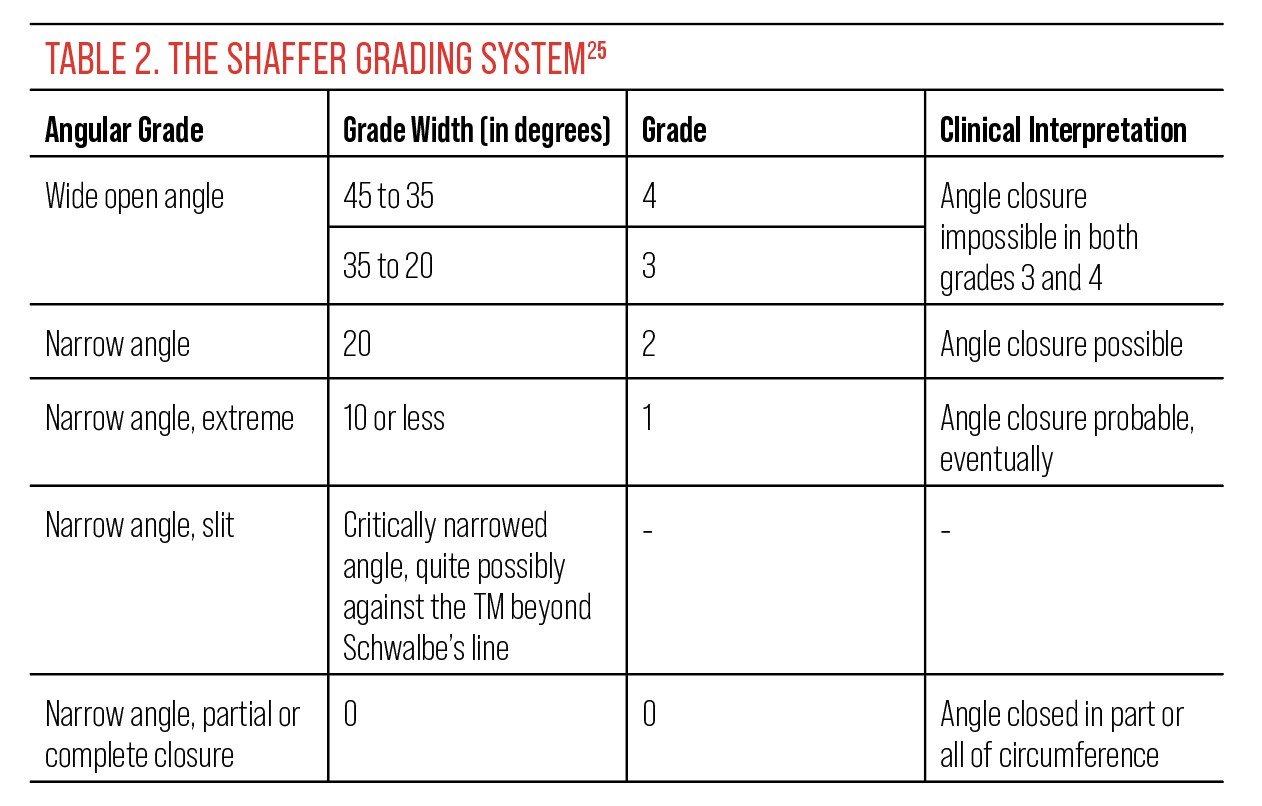 |
The Shaffer gonioscopy grading system attempts to describe the degree of the iris in relation to the TM (Table 2).24 Therefore, a larger grading indicates a wider degree of openness. With this grading system a narrow angle is assigned a grade 2, indicating approximately 20° of opening.
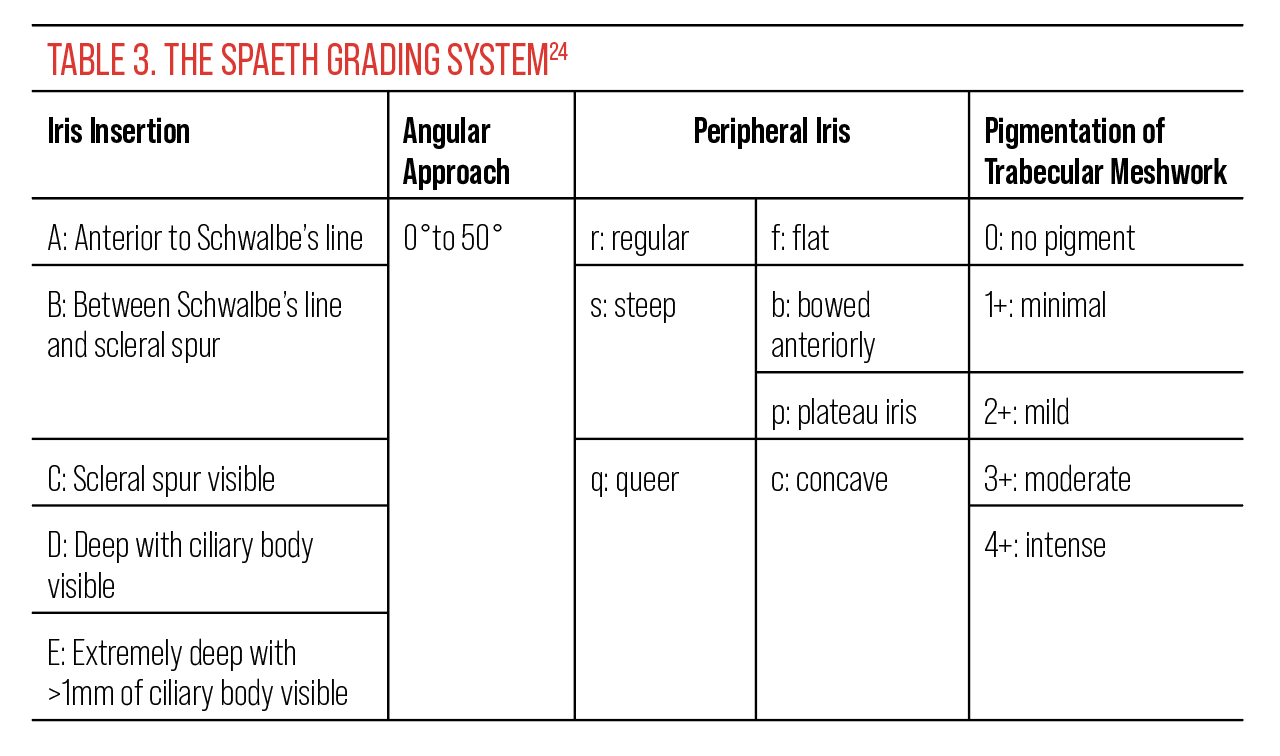 |
The Spaeth grading system describes four clinical aspects of the angle: level of iris insertion, angular width, iris configuration and pigmentation (Table 3). Iris insertion is represented by letters A to E, in which A represents the iris inserting anterior to Schwalbe’s line, B represents insertion anterior to posterior TM, C is posterior to scleral spur, D is “deep” into the ciliary body and E is “extremely” deep with wide ciliary body visibility. The Spaeth grading system lends additional value in the assessment of narrow angles. It denotes parentheses to differentiate the optical insertion vs. the true anatomical insertion revealed by indentation gonioscopy. This technique can expose hidden anomalies that may otherwise be obscured in narrow angles such as angle recession or a plateau iris configuration.
In Spaeth grading, the angular width is more descriptive of the iris approach to the recess rather than the angle of the recess itself.24-25 There are four iris configurations in the Spaeth grading system: “b” denotes a steep anterior bowing of the iris, which can further be broken down on a 1 to 4+ scale; “p” indicates a plateau configuration, which previous grading systems were unable to differentiate; “f” is for flat configurations; and “c” suggests a concave or posterior bowing more consistent in pigment dispersion syndrome. Pigmentation can also be denoted on a numerical scale from 0 (little pigment) to 4+ (heavy TM pigmentation).
Now that we’ve reviewed the basics of angle assessment and anatomy, PACG prevalence and risk factors and the three gonioscopy grading systems, let’s apply this information to help determine the proper course of assessment and diagnosis in another patient case.
Case Two: Patient with high IOP referred for glaucoma evaluation
A 63-year-old Caucasian male was referred by his optometrist to the Glaucoma Institute of State College for management because of an IOP of 28mm Hg OD and 17mm Hg OS with nerve fiber layer thinning on OCT OD. He had a vitrectomy and epiretinal membrane peel six months prior OD. One month after the repair, he developed ocular hypertension and was treated with Cosopt BID OD by the retinal specialist. His corneal-compensated IOP by Ocular Response Analyzer was 24.2mm Hg OD and 20.3mm Hg OS. Corneal hysteresis was reduced at 9.3mm Hg and 9.5mm Hg, and his central corneal thicknesses measured 554µm and 548µm.
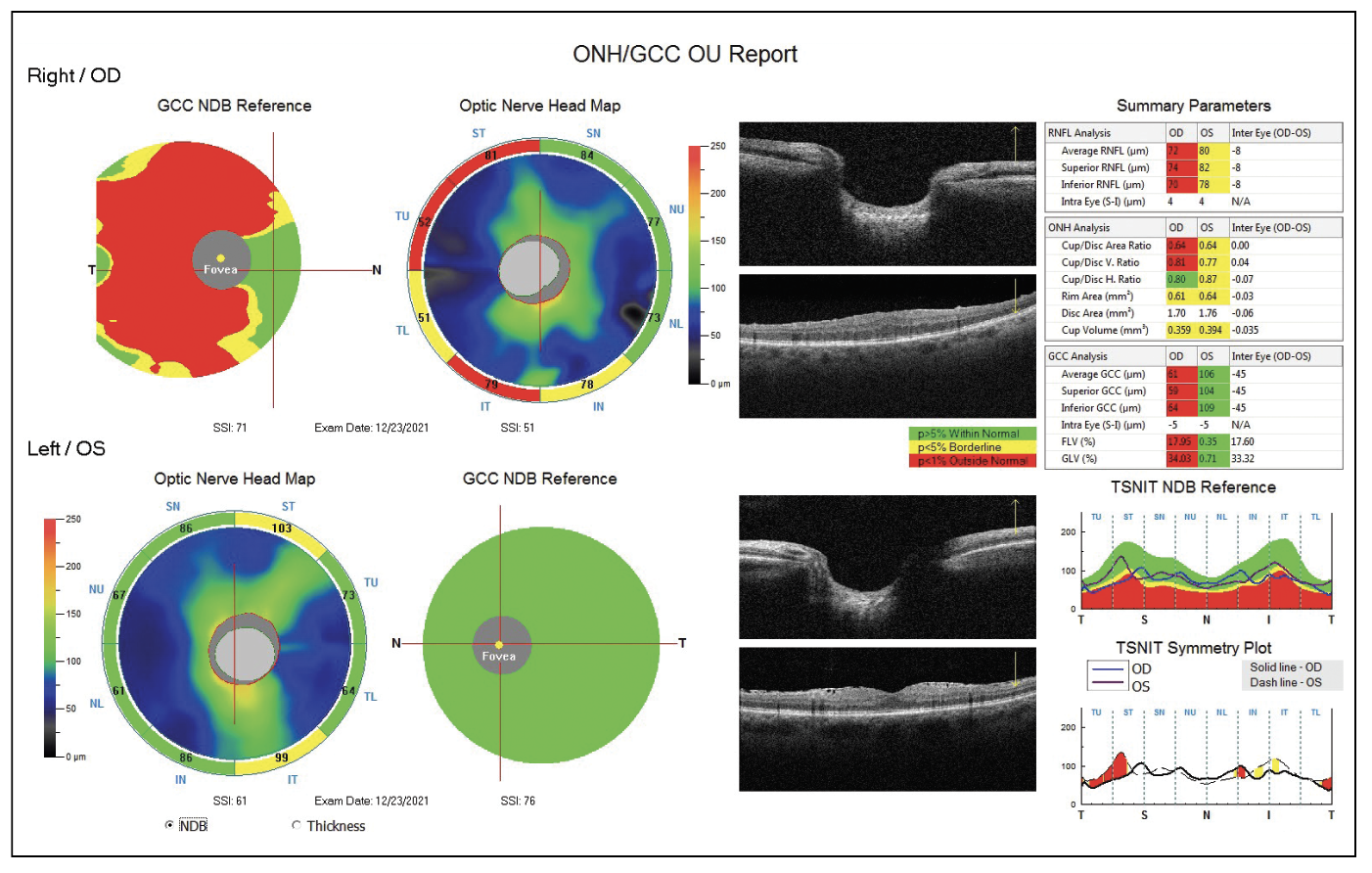 |
Fig. 4. OCT shows a reduced ganglion cell complex and nerve fiber layer in the patient from case 2. Note the significant asymmetry in the ST and IT sectors in the TSNIT Symmetry Plot. Click image to enlarge. |
Should we dilate? Due to the importance of proper nerve and nerve fiber layer assessment, and because he was dilated numerous times by the retina specialist, we felt it was reasonable to dilate. As in case one, gonioscopy should be performed prior to dilation. Gonioscopy revealed minimal posterior TM OD with close to 360° of iridotrabecular contact, which was confirmed by angle OCT (Figure 3A). There were several areas of PAS. Gonioscopy OS showed greater than 180° of iridotrabecular contact with minimal PAS. Cup-to-disc ratios were estimated to be 0.7/0.8 OD and 0.5/0.5 OS, and there was an epiretinal membrane present OS. OCT showed severe glaucomatous thinning of the nerve fiber layer and ganglion cell complex OD (Figure 4).
Post-dilation IOPs measured 31.2mm Hg OD and 23.6mm Hg OS. The patient’s visual fields revealed a superior arcuate defect OD, while OS had scattered nonspecific defects.
Based on the clinical assessment, this patient was diagnosed with chronic moderate-stage PACG OD and PACS OS. We instilled one drop of brimonidine OU prior to sending him home. As in the previous case, we educated him on the symptoms of an angle-closure attack and gave him the number of our on-call service.
Should we perform or recommend LPI or proceed directly to cataract extraction? To help answer this question, let’s take a look at the data from the Effectiveness in Angle-closure Glaucoma of Lens Extraction (EAGLE) study, which recruited 419 patients. One eye was randomized to early lens replacement vs. conventional management in patients with mild to moderate PACG.26 All PAC patients had IOPs above 30mm Hg, and the PACG patients had IOPs above 21mm Hg. While many had early cataracts, all were visually asymptomatic. The study found that patients who had early cataract surgery reduced the need for additional glaucoma surgeries or IOP-lowering medications. They also had a better quality of life and a high chance of being cost-effective at three years.25
Based on the EAGLE study findings and the unlikely success of LPI with PAS, we proceeded directly to cataract surgery and attempted goniosynechialysis and goniotomy on the patient in case one. Goniosynechialysis involves pushing down on the peripheral iris for the purpose of gently removing the iris from the TM, while goniotomy involves removing three to four clock hours of TM. The patient underwent successful cataract surgery with goniosynechialysis and goniotomy OD. Postoperative IOP on Combigan BID was 14.4mm Hg, and OCT showed a more open angle (Figure 3B).
Takeaways
Caring for patients across the angle-closure spectrum may seem challenging. Remember that gonioscopy should always be performed prior to dilation when narrow angles are suspected. Consider LPI if the patient mentions symptoms of angle closure, has a family history of angle-closure disease, has at least +3D of hyperopia or needs frequent dilation. Consider cataract surgery early in patients with PACG.
Having a thorough understanding of PACS, PAC and PACG helps clinicians to know when to recommend or perform dilation, gonioscopy, LPI and cataract surgery, leading to better patient outcomes.
Dr. Cymbor is the medical director of the Glaucoma Institute of State College, a member of the Optometric Glaucoma Society and a managing partner at Nittany Eye Associates.
Dr. Seitz currently works for University Eye Associates, a private group practice in Charlotte, NC, and has a special interest in managing glaucoma and ocular surface disease.
1. Yuan Y, Wang W, Xiong R, et al. Fourteen-year outcome of angle-closure prevention with laser iridotomy in the Zhongshan angle-closure prevention study: extended follow-up of a randomized controlled trial. Ophthalmology. April 6, 2023. [Epub ahead of print]. 2. Lagan MA, O’Gallagher MK, Johnston SE, Hart PM. Angle-closure glaucoma in the Northern Ireland Diabetic Retinopathy Screening Programme. Eye. 2016;30(8):1091-3. 3. Wilensky JT, Kaufman PL, Frohlichstein D, et al. Follow-up of angle-closure glaucoma suspects. Am J Ophthalmol. 1993;115(3):338-46. 4. Baskaran M, Kumar RS, Friedman DS, et al. The Singapore Asymptomatic Narrow Angles Laser Iridotomy Study: five-year results of a randomized controlled trial. Ophthalmology. 2022;129(2):147-58. 5. Yoo K, Apolo G, Zhou S, et al. Rates and patterns of diagnostic conversion from anatomical narrow angle to primary angle-closure glaucoma in the United States. Ophthalmol Glaucoma. 2023;6(2):169-76. 6. Li X, Sundquist J, Zöller B, Sundquist K. Familial risks of glaucoma in the population of Sweden. J Glaucoma. 2018;27(9):802-6. 7. Quigley HA. Understanding the problem of angle-closure glaucoma. Glaucoma Today. 2015;30-1. 8. Emanuel ME, Parrish RK, Gedde SJ. Evidence-based management of primary angle closure glaucoma. Curr Opin Ophthalmol. 2014;25(2):89-92. 9. Suwan Y, Jiamsawad S, Tantraworasin A, et al. Qualitative and quantitative evaluation of acute angle-closure mechanisms. BMC Ophthalmol. 2017;17:246. 10. Cymbor M. Angle-closure glaucoma: are you ready? Review of Optometry. Published October 15, 2016. www.reviewofoptometry.com/article/angleclosure-glaucoma-are-you-ready. Accessed June 15, 2023. 11. Foster PJ, Buhrmann R, Quigley HA, Johnson GJ. The definition and classification of glaucoma in prevalence surveys. Br J Ophthalmol. 2002;86(2):238-42. 12. Kumar G, Ichhpujani P, Bhartiya S, et al. The lens and angle closure. J Curr Glaucoma Practice. 2010;4(1):13-20. 13. Kim YK, Yoo BW, Kim HC, Aung T, Park KH. Relative lens vault in subjects with angle closure. BMC Ophthalmol. 2014;14:93. 14. Ritch R. Plateau iris is caused by abnormally positioned ciliary processes. J Glaucoma. 1992;1:23-6. 15. Chakrabarti K, Samant S, Mohapatra R, et al. A comparison of lens parameters in patients with various subtypes of primary angle-closure disease and the normal population: a prospective study. Indian J Ophthalmol. 2022;70(8):2889-94. 16. Moghimi S, Torkashvand A, Mohammadi M, et al. Classification of primary angle closure spectrum with hierarchical cluster analysis. PLoS One. 2018;23;13(7). 17. Cymbor M. Stout N. A practical approach to angle-closure. Review of Optometry. Published July 15, 2020. www.revieweducationgroup.com/ce/a-practical-approach-to-angleclosure. Accessed June 15, 2023. 18. Sun X, Dai Y, Chen Y, et al. Primary angle closure glaucoma: what we know and what we don’t know. Prog Retin Eye Res. 2017;57:26-45. 19. Boland MV, Zhang L, Broman AT, et al. Comparison of optic nerve head topography and visual field in eyes with open-angle and angle-closure glaucoma. Ophthalmology. 2008;115(2):239-45. 20. Zhang N, Wang J, Chen B, Li Y, Jiang B. Prevalence of primary angle closure glaucoma in the last 20 years: a meta-analysis and systematic review. Front Med (Lausanne). 2021;7:624179. 21. Quigley H, Broman A. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90:262-7. 22. Lee RY, Huang G, Porco TC, et al. Differences in iris thickness among African Americans, Caucasian Americans, Hispanic Americans, Chinese Americans, and Filipino-Americans. J Glaucoma. 2013;22:673-8. 23. Stanley J, Huisingh CE, Swain TA, et al. Compliance with primary open-angle glaucoma and primary open-angle glaucoma suspect preferred practice patterns in a retail-based eye clinic. J Glaucoma. 2018;27(12):1068. 24. Marsh BC, Cantor LB. The Spaeth gonioscopic grading system. Glaucoma Today. 2005;May/June;22-26. 25. Spaeth GL. The normal development of the human anterior chamber angle: a new system of descriptive grading. Transactions of the Ophthalmological Societies of the United Kingdom. 1970;91:709-39. 26. Javanbakht M, Azuara-Blanco A, Burr JM, et al. Early lens extraction with intraocular lens implantation for the treatment of primary angle closure glaucoma: an economic evaluation based on data from the EAGLE trial. BMJ open. 2017;7(1):e013254.24. |
