 |
|
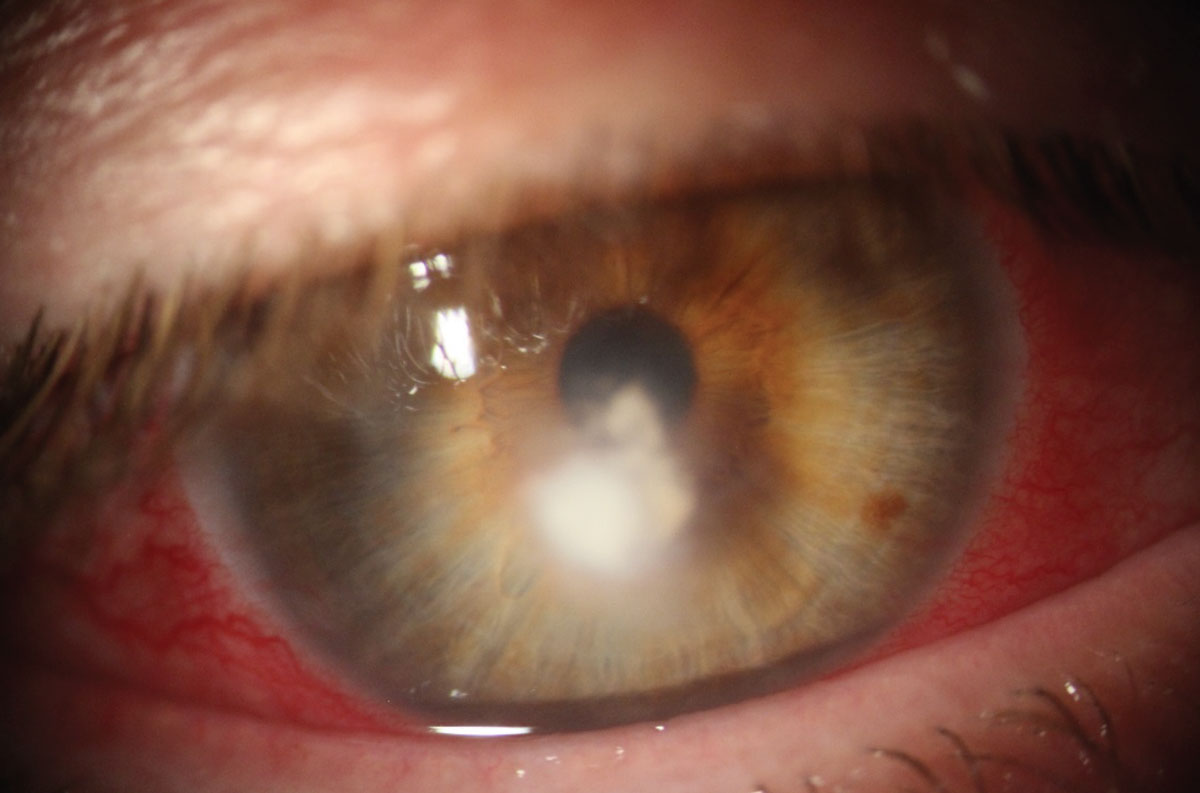
According to the study, Candida species was identified in 96% of yeast keratitis cases while Aspergillus (32%) and Fusarium (26%) were the most common species identified with filamentous patients. Photo: Delaney Kent, OD. Click image to enlarge. |
Fungal keratitis is rare, with a 2022 incidence of in North America of 0.03 cases/100,000 people. While that’s fortunate as a public health matter, the dearth of cases makes it difficult to detect trends in the condition’s epidemiology, and patients and physicians often miss early signs and symptoms of infection due to lack of familiarity. To better understand the trends and clinical outcomes of fungal keratitis, researchers in Canada recently conducted a 20-year study. Here are the methods and results they reported.
Researchers examined cases of yeast and filamentous keratitis from 2003 to 2022, and reviewed factors such as patient demographic, risk factors, visual acuity and treatments. A total of 138 patients (138 eyes), divided evenly between males and females, were involved in the study. There were 75 patients (54%) diagnosed with yeast keratitis and 63 patients (46%) diagnosed with filamentous keratitis.1 Corneal scrapings were performed on each patient at approximately 21 days after symptom offset.
The most common risk factors identified for fungal keratitis in this study were ocular surface disease, contact lens (CL) wear, topical steroid use, topical antibiotic use and previous ocular surgery. Ocular surface diseases were more prevalent in patients with yeast-based keratitis compared to the filamentous group (79% vs. 28%). The most frequent ocular surface disease identified in both groups was herpes simplex virus keratitis (n=16).
Contact lens wear has long been recognized as a risk factor for fungal keratitis.2 This activity was found to be more associated with filamentous-based species than yeast-based infectious organisms (78% vs. 19%). Of the 138 cases, 45% of patients were contact lens wearers, including both bandage lens and refractive correction uses, and CL-related cases “were most common during the years with the highest incidence of fungal keratitis, from 2016 to 2019,” stated the researchers in their study, published in American Journal of Ophthalmology.
About 25% of patients reported overnight wear of their contact lenses, and 17% also engaged in water-contact while wearing lenses (e.g., swimming, showering, hot tub use). Interestingly, refractive CL wear was significantly more common in cases of Fusarium keratitis than bandage lens wear (47% vs. 17%). No increase in CL-related cases overall were observed over the study period.
“In patients that had yeast as the causative organism, topical antibiotic and steroid use, recent healthcare contact and immunosuppression were additional risk factors as compared to patients with filamentous keratitis,” the researchers wrote. Most patients in the study were treated with either 0.15% amphotericin B (29%), 1% voriconazole (25%) or both (11%), while other topical treatments included 2% fluconazole (3.6%), 0.5% caspofungin (0.7%) or 2% ketoconazole (1.4%).
After treatment, visual acuity was assessed. Patients with filamentous keratitis showed a significant improvement in visual acuity (~20/500 Snellen to ~20/250 Snellen) while patients with yeast keratitis did not improve and in fact worsened (~20/1260 Snellen to ~20/1590 Snellen).
“There are several limitations to this study given its retrospective nature,” mentioned the researchers in their study. For one, “A multi-decade study time may not have included all cases that occurred during this period.” The method used for diagnosing fungal keratitis (corneal scraping), which could have been improved using confocal microscopy and corneal biopsy, was also seen as a limitation, and the incidence could have been affected by detection techniques that had advanced over the 20-year study.
“Given that these observations have occurred in a geographic area characterized by temperate and continental climate, the ophthalmological community should maintain a high level of suspicion for fungal keratitis in patients with contact lens-related infections not responding to standard empirical treatment,” concluded the researchers in their paper. “Further research would be needed to elucidate the mechanisms underlying this long-term shift in fungal ecology and risk factors, and to possibly define preventative public health strategies.”
1.Ling JYM, Yeung SN, Chan C, et al. Trends and clinical outcomes of fungal keratitis in Canada: A 20-year retrospective multicenter study. Am J Ophthalmol. April 14, 2024. [Epub ahead of print]. 2. Ong HS, Fung SSM, Macleod D, et al. Altered patterns of fungal keratitis at a london ophthalmic referral hospital: An eight-year retrospective observational study. Am J Ophthalmol. 2016;168:227-236. |