 |
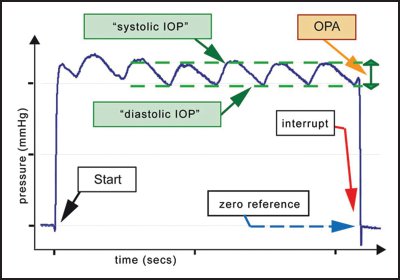
| Ocular pulse amplitude tracks changes in IOP that stem from blood pressure dynamics to better characterize intraocular pressure. Photo: Ziemer. Click image to enlarge. |
Tracking intraocular pressure (IOP) over time is key for estimating risk of progression as well as response to treatment. However, diurnal IOP fluctuation is a well-known phenomenon and a source of some consternation in clinical practice, as it degrades the accuracy of pressure-based analysis of the case. Does it have any correlation with disease prognosis? British researchers recently evaluated whether IOP fluctuation is independently associated with visual field progression rates, as the literature on the effects of IOP fluctuation is conflicting. Their results, published recently in Ophthalmology, suggested that IOP fluctuation wasn’t associated with progression.
The double-masked, multicenter trial included 217 patients and 213 placebo participants with five or more visual fields. Normalized IOP fluctuation variables included ocular pulse amplitude (OPA)—the difference between diastolic and systolic IOP—and diurnal and long-term IOP fluctuation. Non-fluctuation variables included baseline, peak, mean, supine and peak phasing IOP, which were combined using principal component analysis, a technique using best-fit directions (principal component 1) in a linear coordinate system.
Corneal ConfoundersThe authors investigated some non-IOP-related ocular factors in their Ophthalmology paper and noted that the role of central corneal thickness (CCT) is often “misunderstood.” Why? A thinner cornea, they explained, can cause applanation tonometry artifacts, yielding an IOP underestimation. Additionally, corneal thickness may be a biomarker for the biomechanics of the lamina cribrosa and peripapillary sclera, thereby giving information about the optic nerve and not IOP. “In our cohort, thinner CCT was associated with faster progression rates in some multivariable models (which included IOP metrics), while it didn’t show significance in any of the univariable models,” they wrote. “This suggests that CCT alone is not directly associated with glaucoma progression: rather, it becomes statistically significant when measured IOP is included in the model due to the effect of CCT on measured IOP.” Similarly, they wrote that corneal hysteresis “is inversely related to IOP. Therefore, low corneal hysteresis may reflect high IOP, which is an established risk factor for faster glaucoma progression” and is also “directly related to corneal stiffness and thickness. Hence, IOP might have [been] underestimated in patients with low corneal hysteresis, with consequent undertreatment leading to faster progression.” |
The researchers reported that in the placebo arm of the trial, only principal component 1 (PC1), and no normalized IOP fluctuation metrics, demonstrated a significant association with the mean deviation rate (estimated at -0.19 dB/year). In the treatment arm, no variables were significantly associated with mean deviation rates. They also found that for the fastest five locations in the placebo group, PC1 (-0.58 dB/year), central corneal thickness (0.26 dB/year for 10 µm thicker) and normalized OPA (-3.5 dB/year) were associated with rates of progression. Normalized diurnal IOP fluctuations and long-term IOP fluctuations were not associated with rates of progression. Only PC1 (-0.27 dB/year) was associated with rates of progression in the treatment group.
The researchers concluded that their study “finds no evidence to support that either diurnal or long-term IOP fluctuation, defined in a clinically relevant manner, are independent factors for glaucoma progression.” They added that “other aspects of IOP, such as mean IOP and peak IOP, may be more informative. Higher OPA may be an independent factor for faster glaucoma progression.”
Rabiolo A, Montesano G, Crabb DP, et al. Relationship between intraocular pressure fluctuation and visual field progression rates in the United Kingdom Glaucoma Treatment Study. Ophthalmology 2024. [Epub ahead of print]. |
