 |
A 17-year-old woman presented with a chief complaint of headache and pain in upgaze of four months’ duration. She explained her vision was good and she realized the issue was getting worse over the last three weeks. Her GP scheduled her to see a neurologist and asked her to see the eye doctor. She denied trauma and took no medications. She denied allergies of any kind.
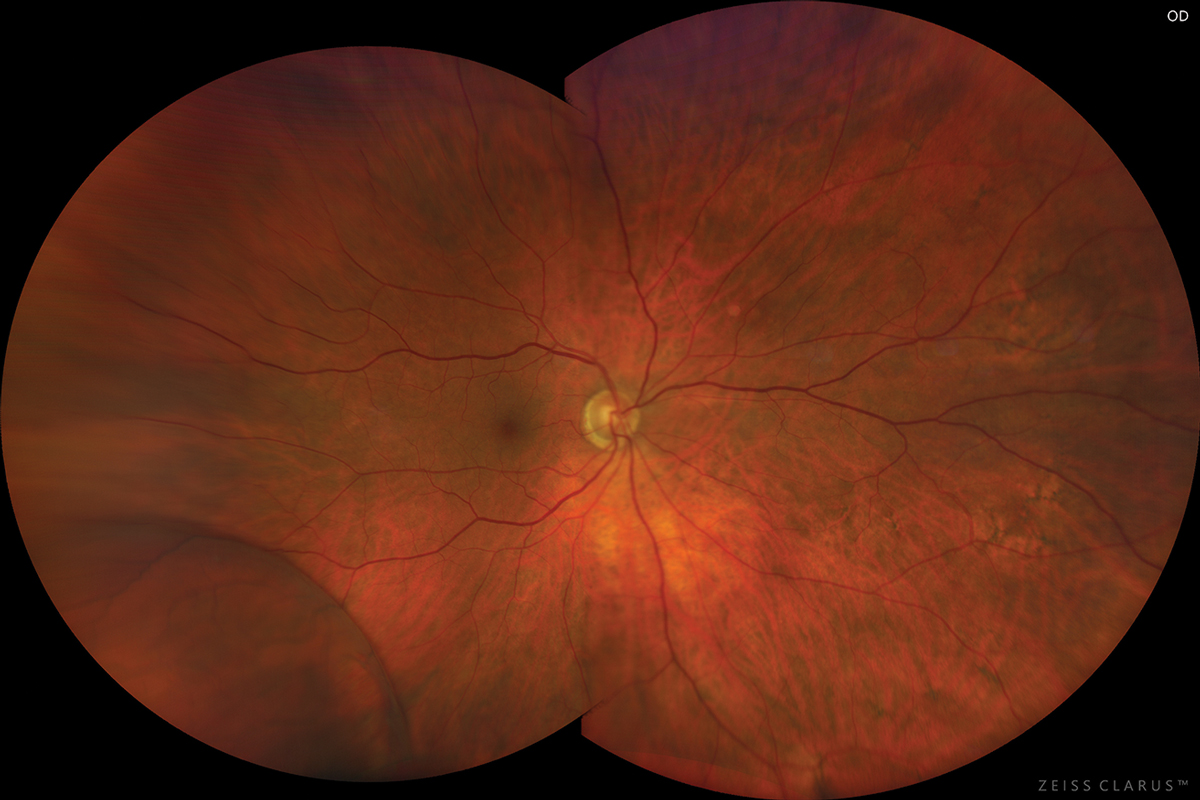
Best-corrected acuities were 20/20 OD and OS at distance and near. Her external exam found pain upon looking upward in any direction with no limitation of upgaze and no diplopia. There was no afferent pupillary defect. Confrontation fields were full. Anterior segment findings were normal. Goldmann tonometry measured 17mm Hg OU. Dilated fundus exam demonstrated normal-appearing cup disc/ratios measuring 0.3/0.3 round, with sharp and pink discs.
 |
| The patient had no restriction of upgaze but reported pain during the experience. Click image to enlarge. |
The superior adnexa and orbital rim were palpated, with particular attention paid to the region housing the trochlear fossa, notch and tendon. All other directions of gaze were tested for pain or limitation of motility and diplopia. Exophthalmometry was done to rule out proptosis. The eye was closely inspected for inflammation (iritis, episcleritis). Color and brightness were assessed to ensure there was no evidence of optic neuritis. The fundus was observed for signs of any mass effect (choroidal folds) and papilledema was ruled out by observation of the cup/disc with sharp margins and the identification of a spontaneous venous pulse.
Pathophysiology and Workup
The estimated prevalence of trochleitis according to one report in the literature is 12 per 100,000.3 The average age of onset varies in the literature with an average of 43 years (+/- 15).3,4 The majority of cases occur in women.3,4
The sensory innervation of the trochlear region of the orbit is innervated by a branch of the ophthalmic division of the trigeminal nerve.5 This permits modulatory influences over the nociceptive afferents of the region during episodes of migraine headache.5 Migraine headache can provoke regional trochlear pain (known as “trochlear migraine”). The pain may be an associated complication of the migraine headache or the migraine headache may have evolved secondary to the trochlear region pain. When the painful area is in the vicinity of the trochlear notch, it is referred to as “trochleodynia.”5
“Trochleitis” is the term used to connote an inflammatory trochleodynia unrelated to the vasospastic etiology. Trochleitis is generally idiopathic but can be associated with the usual immunologic and rheumatologic suspects, whih include lupus erythematous, rheumatoid arthritis, juvenile idiopathic arthritis, Bechet’s disease, sarcoidosis, syphilis, tuberculosis, lymphoma, Still’s disease (fevers, variable salmon-colored rash and arthritis, sometimes referred to as “systemic-onset juvenile idiopathic arthritis”) and paranasal sinusitis.1,5-10
In cases of trochleitis, trigeminal neurons become sensitized by the friction created when the superior oblique tendon passes through the trochlear sling.8,9 The chronic microtrauma results in stenosing tenosynovitis.8,9 Perivascular lymphocytic infiltration of connective and adipose tissues adjacent to trochlear cartilage occurs along with some invasion into the superior oblique myofibrils as demonstrated via biopsy.11 The resultant headache may exist on its own or can provoke/exacerbate a migraine headache.5,8,9-11 This is also what creates the palpation tenderness.1-11 Chronic trochleitis has been associated with trochlear tendon abnormalities and motility obstruction. This is known in the literature as Brown’s syndrome associated with trochleodynia.
Trochleodynia/trochleitis is a diagnosis of exclusion based on clinical findings. “Doll’s eye” motilities can be completed to ensure the findings are consistent and repeatable. While the likelihood is small, cases of unilateral trochleitis deserve consideration for a basic medical work-up including testing for rheumatoid arthritis, juvenile arthritis, Bechet’s disease, sarcoid, tuberculosis, syphilis and lupus. Bilateral or repeat cases and cases in young patients (<10 years) mandate testing, as trochleitis has been documented to be the initial presenting sign of evolving latent systemic disease.1,10 Regional swelling and inflammatory changes can also be demonstrated on radiologic evaluations such as computerized tomography (CT), magnetic resonance imaging (MRI) and ultrasonography; however, because the tissues being evaluated are small, lack of radiologic evidence does not preclude the diagnosis.1,8,11
 |
|
This photo of a different patient with the same condition shows a comparable presentation. Photo: Jay M. Haynie, OD. Click image to enlarge. |
Treatment Considerations
Management of the systemic disease is a critical component to longstanding resolution of the ocular signs and symptoms.1-3,7-10
Trochleitis can be managed with oral NSAIDs.1-12 They are a reasonable first option that are well tolerated with fewer side effects than their oral steroidal counterparts. Oral steroids can be added in cases requiring additional immunologic suppression.1-12 Immunosupressive medications are another option that can be added or substituted.9Peritrochlear steroid injection can be ordered in recalcitrant cases or for instances where repeated inflammation threatens to produce Brown syndrome.6,12
This patient was referred to their internal medicine doctor for a physical, blood work and the initiation of oral non-steroidal medications by mouth. The laboratory work-up returned negative and her condition resolved over three weeks.
Dr. Gurwood is a professor of clinical sciences at The Eye Institute of the Pennsylvania College of Optometry at Salus University. He is a co-chief of Primary Care Suite 3. He is attending medical staff in the department of ophthalmology at Albert Einstein Medical Center, Philadelphia. He has no financial interests to disclose.
|
1. Tran TM, McClelland CM, Lee M. Diagnosis and management of trochleodynia, trochleitis, and trochlear headache. Front Neurol. 2019;10(4):361. 2. Smith JH, Garrity JA, Boes CJ. Clinical features and long-term prognosis of trochlear headaches. Eur J Neurol. 2014;21(4):577-85. 3. Jarrín E, García-García Á, Hurtado-Ceña FJ, Rodríguez-Sánchez JM. Clinical characteristics, treatment, and outcome of trochleitis. Strabismus. 2017;25(1):1-4. 4. Chanlalit W, Teeyapant C, Soodchuen S. Trochlear pain: clinical characteristics and treatment outcomes. J Neurol. 2018;265(2):376-80. 5. Pareja JA, Sánchez del Río M. Primary trochlear headache and other trochlear painful disorders. Curr Pain Headache Rep. 2006;10(4):316-20. 6. Giannaccare G, Primavera L, Maiolo C, et al. Steroid intra-trochlear injection for the treatment of acquired Brown syndrome secondary to trochleitis. Graefes Arch Clin Exp Ophthalmol. 2017;255(10):2045-50. 7. Gutmark R, Eliasieh K, Rivera-Michlig R. A case of bilateral trochleitis in adult-onset Still's disease. Semin Arthritis Rheum. 2014;43(5):689-91. 8. Hong H, Lyu IJ. Pediatric trochleitis associated with paranasal sinusitis: a case report. BMC Ophthalmol. 2019;19(1):16. 9. Pareja JA, Sanchez del Rio M. Primary trochlear headache and other trochlear painful disorders. Curr Pain Headache Rep. 2006;10(4):316-20. 10. Fonseca P, Manno RL, Miller NR. Bilateral sequential trochleitis as the presenting feature of systemic lupus erythematosus. J Neuroophthalmol. 2013;33(1):74-6. 11. Tychsen L, Tse DT, Ossoinig K, Anderson RL. Trochleitis with superior oblique myositis. Ophthalmology. 1984;91(9):1075-9. 12. Zaragoza-Casares P, Gómez-Fernández T, Gómez de Liaño MA, Zaragoza-Garcia P. Bilateral idiopathic trochleitis as a cause of frontal cephalgia. Headache. 2009;49(3):476-7. |
