Trouble at the SurfaceMedication, infection, genetics, poor hygiene—these are only a few factors that contribute to ocular surface health. This month in Review of Optometry, experts weigh in on the pathophysiology, diagnosis, treatment and management of numerous diseases affecting this delicate part of the eye. |
Eye drops intended to lower intraocular pressure (IOP) are often chosen as first-line therapy for primary open-angle glaucoma (POAG), as the medication is generally effective and well-tolerated with good safety profiles. Of the various side effects associated with these topical therapies, symptoms and clinical signs involving the ocular surface are among the most common reported by patients and clinicians.
Mitigating these side effects is an important responsibility of the clinician, as they can be troublesome in patients’ everyday activities. Not only does this increase patient satisfaction and quality of life, but it likely increases compliance. Before discussing mitigation tactics, we first need to understand the mechanisms of ocular surface disease on a pathophysiological level. Each class of pressure-lowering eye drops has its own set of ocular surface-associated side effects and different mechanisms of action.
Prostaglandin Analogs
Of all the topical IOP-lowering medications, prostaglandin analogs are the class most commonly prescribed as a first-line therapy for POAG. They are typically the most efficacious option—on average, prostaglandin analogs lower IOP by 30%.1 This class of drugs includes latanoprost, latanoprostene bunod, travoprost, bimatoprost, tafluprost and the combination drop Rocklatan (netarsudil + latanoprost ophthalmic, Aerie Pharmaceuticals). The use of prostaglandin analogs can cause ocular surface side effects, including conjunctival hyperemia and dry eye disease.2,3
The active agents in prostaglandin analogs are thought to cause dilation of conjunctival blood vessels, leading to conjunctival redness, which is a relatively simple explanation.4 Conversely, there are many more theorized mechanisms by which prostaglandin analogs may cause dry eye symptoms. First, prostaglandin analogs can induce tear film instability through a few differing processes. These drugs cause a local inflammatory response within the trabecular meshwork, contributing to their intended effect of lowering IOP. However, this local inflammatory response also occurs on the ocular surface.5 Consequently, these changes in concentration of inflammatory mediators can be enough to destabilize the tear film.
Additionally, this class of drugs has the potential to affect the production of every layer of the tear film. Mucin-producing cells within the conjunctiva are particularly sensitive to inflammation, so chronic exposure to prostaglandin analogs may also cause a decrease in mucin quality and quantity over time, thereby further impacting tear film stability.2,3,5 Local inflammation can occur at the lid margin, leading to thickening and blockage of the meibomian gland ducts; this obstructive meibomian gland dysfunction could then lead to evaporative dry eye.2,4
 |
|
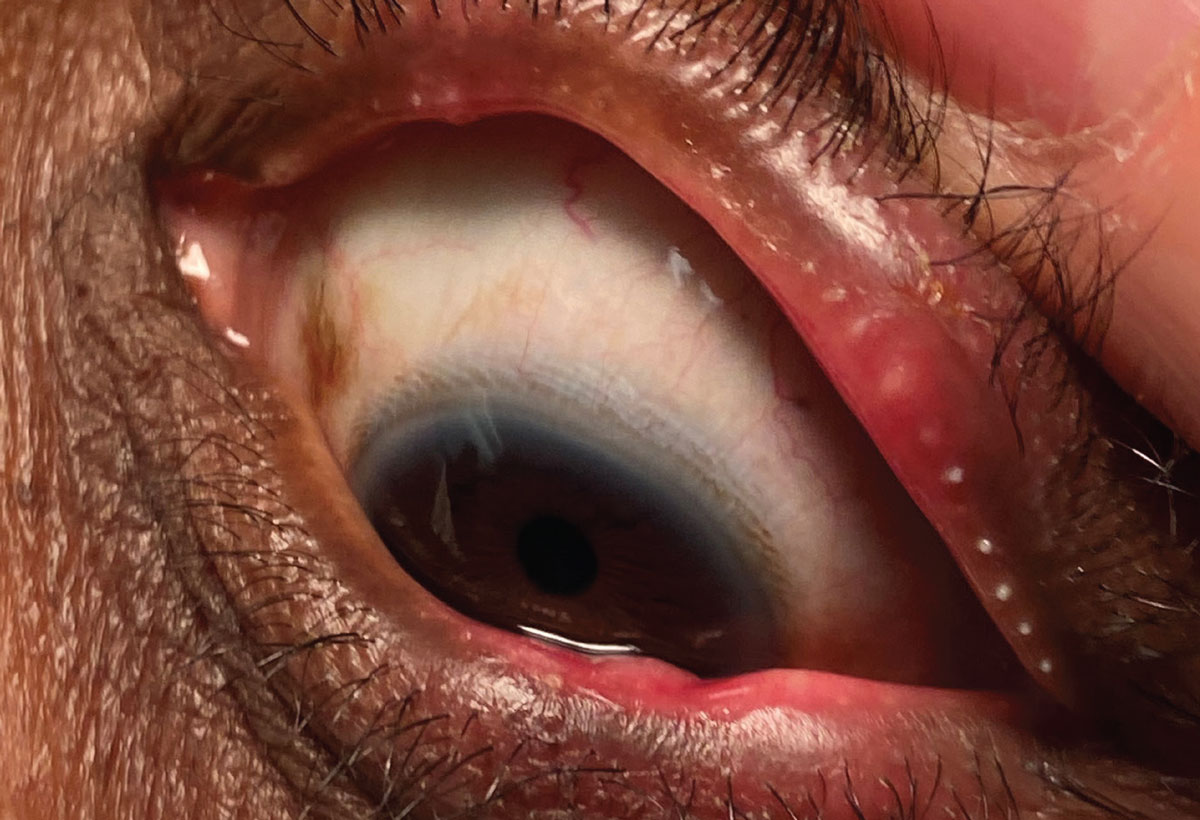
Severe obstructive MGD with gland inspissation and lid margin scalloping. Click image to enlarge. |
Topical prostaglandin analogs may also affect aqueous tear volume. Increased uveoscleral outflow of aqueous, a mechanism by which these medications lower IOP, also affects the osmotic dynamics of the eye and may potentially lead to decreased tear volume. Prostaglandin analogs can alter the flow of blood to the lacrimal glands as well as cause inflammation to them—both processes having the potential to reduce lacrimal gland function, consequently reducing aqueous tear production.6,7
Beta Blockers
The most commonly used IOP-lowering beta blockers include timolol and two combination drops—Combigan (brimonidine tartrate + timolol maleate ophthalmic, Allergan) and Cosopt (dorzolamide hydrochloride + timolol maleate ophthalmic, Thea). The active beta blocker component in this class of medications can sometimes cause local allergic reactions, corneal hypoesthesia and its sequelae and dry eye symptoms.8,9
Beta blockers have a multifactorial effect on the autonomic nervous system’s control of tear secretion. They cause a reduction in the sympathetic production and secretion of the aqueous component of tears by blocking beta-2 adrenergic receptors on the lacrimal gland.10 This imbalance of the sympathetic and parasympathetic activity in the lacrimal glands leads to decreased sensitivity to acetylcholine, the parasympathetic neurotransmitter that stimulates the lacrimal glands to produce tears.
Alpha Agonists
Topical alpha-2 adrenergic agonists used to treat glaucoma include brimonidine, apraclonidine, and two combination drops—the already mentioned Combigan and Simbrinza (brinzolamide + brimonidine tartrate ophthalmic, Alcon). Documented ocular surface side effects of this class are often allergic in nature, causing conjunctival hyperemia, itching and foreign body sensation.8,10,11
Another documented side effect is punctate keratopathy, which may manifest as punctate epithelial erosions or epithelial microcysts.8,9 Punctate keratopathy in this case may be caused by an inflammatory response to the active agent as well as tear film instability. Regarding the latter, although the mechanisms are not perfectly understood, there are likely a few factors at play. For one, alpha agonists can decrease the amount of acetylcholine release in the lacrimal glands, thus decreasing tear volume. They can also decrease corneal nerve sensitivity, which will decrease the cornea’s ability to recognize dryness or irritation and adequately signal this information to the lacrimal gland for needed tear production.10,12,13
 |
|
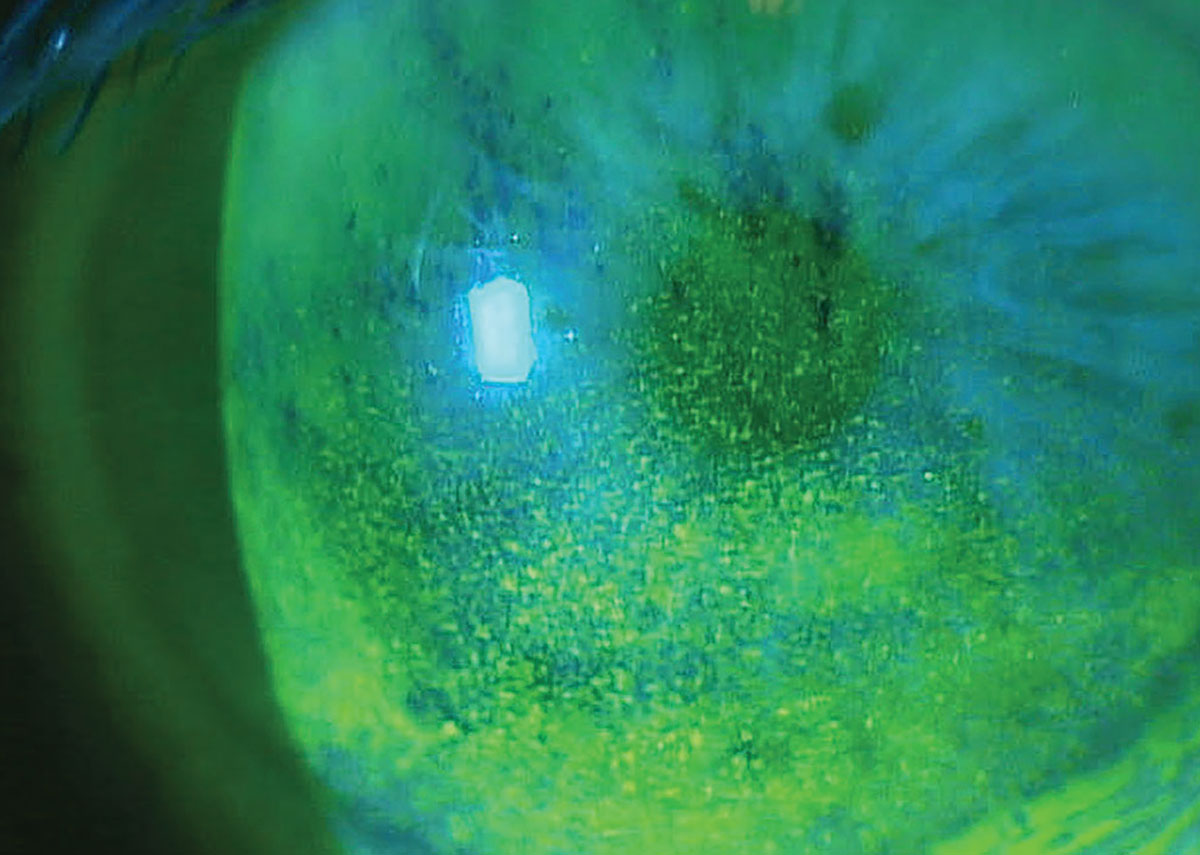
Superficial punctate keratitis in a patient on multiple topical glaucoma medications. Photo: Paul M. Karpecki, OD. Click image to enlarge. |
The mechanism of corneal epithelial microcyst formation is also not fully understood, but it is believed that the direct binding of alpha agonists to corneal epithelial cells results in changes in cell-to-cell adhesions, allowing fluid to flow more readily into intracellular spaces in the epithelium. This direct binding may also affect epithelial cell migration and turnover, leading to irregular cell orientation and spacing, therefore also leading to fluid-filled intracellular spaces. Alpha agonists additionally may alter the osmotic gradient between the tear film and corneal epithelial cells, causing a flow of fluid into cells which then may lead to microcysts.8,9,12
Carbonic Anhydrase Inhibitors
Topical CAIs used to manage glaucoma include dorzolamide, brinzolamide and the two combination drops of Cosopt, also a beta blocker, and Simbrinza, also an alpha agonist. Documented corneal side effects of CAIs include local allergic reactions and mild punctate keratopathy.10,14 The mechanism responsible for the development of punctate keratopathy is not fully understood but is likely multifactorial.
Drugs in this class alter the pH of the tear film.8,10 When the carbonic anhydrase enzyme is inhibited, formation of bicarbonate ions decreases. The tear pH becomes dysregulated, which can cause corneal epithelial disruption. This disruption may then impair the barrier function of the corneal epithelium, disrupt ion transport across the corneal epithelium, change cellular adhesion within the epithelium and may impact the osmotic effects between the cornea and the tear film. It is also hypothesized that all of these insults to the corneal epithelium’s integrity and cornea’s hydration can have a negative influence on corneal nerve sensitivity. As discussed in the section on alpha agonists, decreasing corneal nerve sensitivity leads to a less ability of the cornea to recognize dryness or irritation. As a result, the signaling of information to the lacrimal glands for tear production is negatively impacted.8,14,15
Rho Kinase Inhibitors
This relatively new class of medications used topically to treat glaucoma include netarsudil and the combination drop Rocklatan. The active component in these can cause local allergic reactions, mild punctate keratopathy and whorl keratopathy.16-18
As with many of these topical glaucoma-mitigating drugs, the mechanism by which topical rho kinase inhibitors may cause the exacerbation or new onset of ocular surface dryness is caused for many reasons. One of which is that they may act on the lacrimal glands in various ways to decrease aqueous tear production.10,17,19 Rho kinase enzymes play a role in smooth muscle contraction. Within the lacrimal glands, there are myoepithelial cells that must contract in order to expel tears from the gland and into the tear duct system. When rho kinase enzymes are inhibited within the lacrimal glands, this contraction is suppressed. This causes an overall decrease in aqueous tear production and thus, an unstable tear film.10,17
Similar to some of the drug classes already discussed, these medications may also cause alterations in corneal epithelial cell behavior.9,10 A crucial function of the rho kinase enzyme within the cornea is regulation of the actin cytoskeleton. This structural framework is comprised of actin filaments and it is present not only within the corneal epithelium, but also in the stroma and the endothelium. The actin cytoskeleton is organized in specific configurations to provide structural stability that can withstand mechanical stress while simultaneously promoting corneal transparency. These actin filaments are also responsible for cell-to-cell adhesion, allowing epithelial cells to adhere to adjacent epithelial cells as well as the underlying basement membrane. This adhesion is an important component of the barrier between the cornea and the external environment.
 |
|
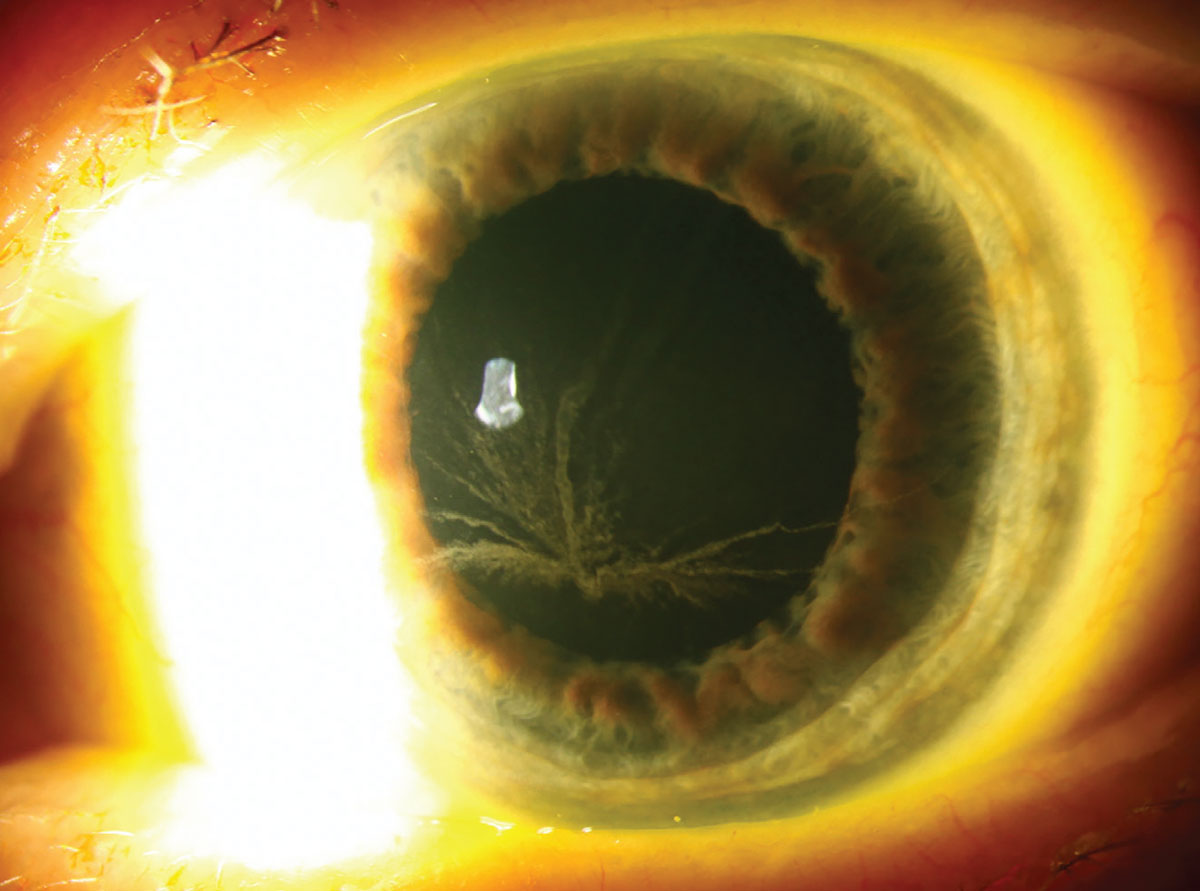
An example of drug-induced corneal verticillata (in a patient on amiodarone therapy). Photo: Christine Sindt, OD. Click image to enlarge. |
What’s more, this actin framework is dynamic and promotes cell migration during corneal wound healing, as well as being responsible for the formation and maintenance of corneal epithelial tight junctions which regulate corneal permeability to ions and water. At the level of the endothelium, a lack of actin would compromise the structures responsible for regulating corneal transparency and hydration. Lastly, the corneal actin filaments are influenced by different signaling pathways to regulate cell shape and function in response to different external stimuli. These many functions of actin are all impacted when rho kinase is inhibited, and a collapse in this structural framework would have a significant impact on the health of the ocular surface at every layer of the cornea and tear film.20
Similar to the effects of prostaglandin analogs, rho kinase inhibitors may also affect corneal nerve function and sensitivity. They may cause localized inflammation of the ocular surface with chronic use that can negatively impact corneal structure and function, and they can cause changes in blood flow throughout the anterior segment of the eye.5,16,17 Compromised anterior segment blood flow may negatively impact the delivery of oxygen and vital nutrients to the cornea.
Whorl keratopathy, also known as vortex keratopathy or corneal verticillata, is characterized by fine deposits appearing in a “whorl”-like configuration within the corneal epithelium. These deposits can be whiteish-gray, yellow or brown in color and are typically located in the inferior-central cornea. This finding can be a sign of various underlying systemic conditions and is also a known side effect of certain medications, including rho kinase inhibitors.21,22
The exact mechanism of drug-induced whorl keratopathy is not fully known. However, some theories suggest that it is an accumulation of metabolic waste due to epithelial cell dysfunction. Fortunately, whorl keratopathy is widely considered a benign finding that does not typically cause any visual or ocular symptoms; most cases can be monitored without intervention. It is reversible with cessation of the responsible agent in visually significant cases.22
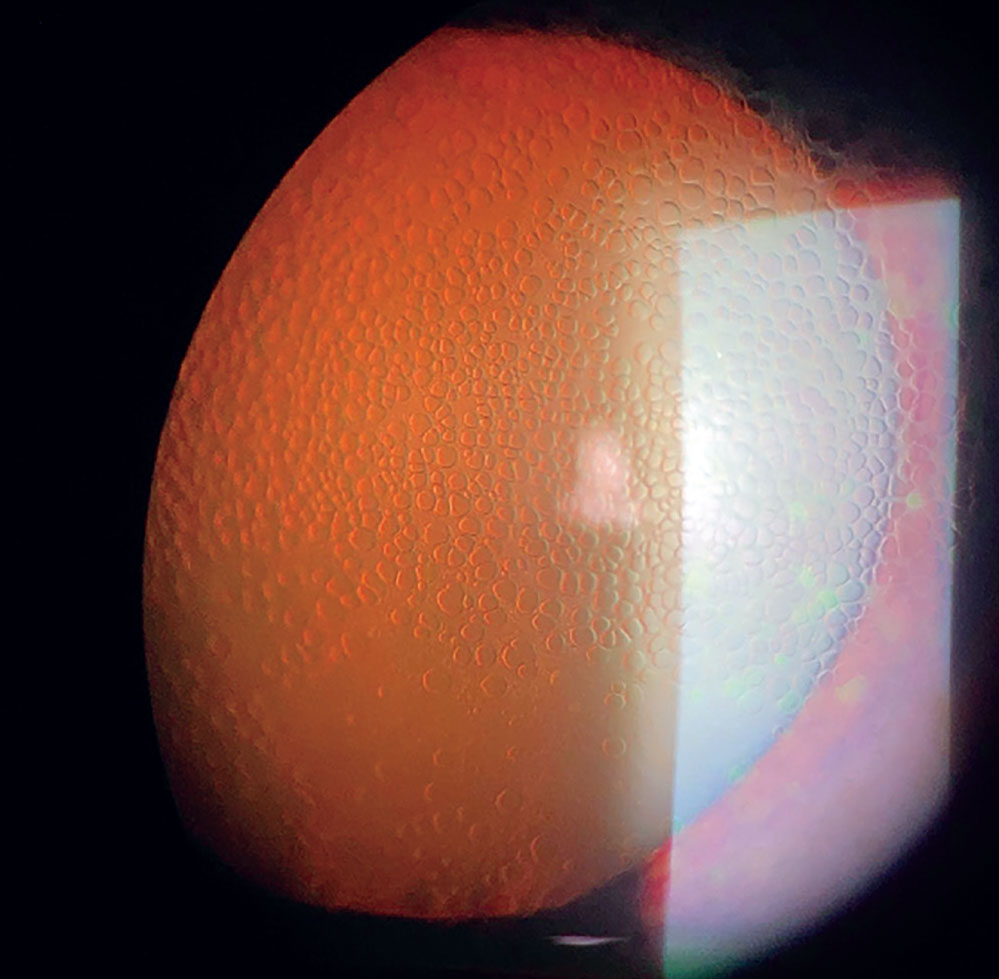
Some patients may exhibit honeycomb corneal edema or reticular corneal edema—side effects unique to rho kinase inhibitors. An adverse reaction like this is more likely to occur in patients with pre-existing corneal edema or corneal endothelial decompensation.23,24
 |
|
Honeycomb corneal edema as a result of topical netarsudil use. Click image to enlarge. |
Benzalkonium Chloride (BAK)
The active components in each class of glaucoma drop mentioned above have their own unique effects on ocular surface health. As discussed, many of these are poorly understood and require more research to determine their clinical significance. This is not the case for BAK, a preservative whose ocular surface side effects are well-documented. BAK is found in many topical ophthalmic medications, including many of the drug classes of drops mentioned above. The adverse effects of this preservative on the ocular surface include corneal and conjunctival cell cytotoxicity and dry eye disease.8-10,25,26
BAK has detergent properties, which allow it to disrupt the lipid layer of the tear film and the lipid bilayer of corneal epithelial cells, both of which processes increase penetration of the BAK-containing medications. This lipid layer disruption is a direct mechanism of corneal and conjunctival cell damage that contributes to ocular surface discomfort. Additionally, breakdown of lipids within the tear film leads to tear instability and, consequently, exacerbation of evaporative dry eye disease.8-10,25,26
Mitigating Adverse Reactions
Not all patients experience adverse effects to these drops or to the preservative of BAK. While clinicians cannot always predict who will be affected, there are factors that may increase a patient’s susceptibility to drug- or preservative-induced corneal toxicity. Patients with pre-existing ocular surface disease, such as dry eye disease, meibomian gland dysfunction and history of chronic conjunctival irritation like allergic conjunctivitis, may already have compromised corneal and conjunctival cell integrity as well as tear film insufficiency and instability. Adding these drops’ agents into this compromised environment has the potential to exacerbate these already suboptimal ocular surface conditions.
With BAK specifically, contact lens wearers sometimes experience greater sensitivity to the preservative for a few reasons. One is that there is potential for an interaction between the preservative and certain contact lens materials. Another reason is the inherent mechanical disruption of the tear film during contact lens use, which may be exacerbated when adding BAK to the patient’s ocular surface. Additionally, BAK sensitivity seems to be dose-dependent and cumulative, meaning that patients who take more frequent doses of BAK-containing medications, who have been using these medications over a longer duration of time and those who take medications that have higher BAK concentrations are all more likely to experience these adverse side effects.
Clinicians may decide to forgo prescribing BAK-preserved medications altogether for patients apart of these susceptible populations. In these cases, one can consider preservative-free formulations or those containing milder preservatives. Such examples include the preservative-free drugs Zioptan (tafluprost ophthalmic, Thea) Cosopt PF (Thea), Timoptic in Ocudose (timolol maleate ophthalmic, Thea) and Iyuzeh (latanoprost 0.005%, Thea), or the mildly preserved options of Travatan Z (travoprost ophthalmic, preserved with Sofzia, Alcon), Alphagan P (brimonidine tartrate ophthalmic, preserved with Purite, Allergan) and Xelpros (latanoprost ophthalmic, preserved with potassium sorbate, Sun Pharmaceutical).9,26,27
Clinicians may also consider limiting overall exposure by only prescribing agents with lower BAK concentrations. Choosing ones that require less frequent dosing is another good option if this can sufficiently control IOP.
If a patient experiences ocular surface side effects with a particular medication, the clinician can consider prescribing a different class of drug with a different mechanism of action. Selective laser trabeculoplasty, sustained-release drug delivery implants or minimally invasive glaucoma surgery may also be considered. These three options typically have a much lower risk of adverse effects involving the ocular surface, as they often minimize the frequency of eye drops, thereby decreasing exposure risk.9 If choosing to keep susceptible patients on these medications, it is important to monitor ocular surface health regularly in order to detect any early signs of toxicity.
Treatment of ocular surface disease in these cases can vary and may involve supplementation with preservative-free artificial tears, opting for lubricating gel or ointment at nighttime, prescribing cyclosporine or lifitegrast eye drops to control ocular surface inflammation, instilling Lumify (brimonidine tartrate ophthalmic, Bausch + Lomb) for redness, stressing the practice of warm compresses and lid hygiene and use of omega-3 or flaxseed supplements.28
The use of punctal plugs is controversial, as many of these drops increase the concentration of inflammatory mediators in the tear film, with increased exposure time potentially making symptoms worse.29 The decision is dependent on which type of drug is causing the symptoms and whether the issue stems from aqueous deficiency, evaporative dry eye or a combination.
Takeaways
Ocular surface irritation is a very common but remediable side effect that has been documented for each class of topical glaucoma medication, with some classes demonstrating more significant or more common side effect profiles than others. Mitigating these side effects while also prioritizing efficacy of the chosen treatment is important in maintaining ocular surface health and, therefore, better chance of patient compliance. We as eyecare clinicians are fortunate to have a plethora of options for glaucoma management: many different ophthalmic drops, BAK-free alternatives and surgeries varying by invasiveness. Looking at the complete clinical picture, each patient will have a different best-fit treatment plan.
We are also armed with many treatments for ocular surface disease that do not exhibit poor interactions with the glaucoma treatments mentioned in this article. The decision to prophylactically treat dry eye disease when prescribing anti-glaucoma medication should be determined on a case-by-case basis. A balance must be struck between maintaining ocular surface comfort and keeping treatment regimens as streamlined as possible to facilitate good compliance. Patients who are identified as being particularly susceptible to adverse ocular surface reactions, as discussed above, can be considered. At the very least, patients should have any pre-existing ocular surface disease under good control, as they are the most susceptible.
Mitigating ocular surface discomfort is significant for a patient’s daily experience and should be a high priority. Ultimately, we owe it to our patients to protect their vision with the best treatment option to provide a satisfactory quality of life.
Dr. Patrizi completed her Doctor of Optometry at the University of the Incarnate Word Rosenberg School of Optometry in San Antonio, Texas. She also completed a residency in ocular disease and primary care at Salus University Pennsylvania College of Optometry, where she is currently an assistant professor.
1. Lee AJ, McCluskey P. Clinical utility and differential effects of prostaglandin analogs in the management of raised intraocular pressure and ocular hypertension. Clin Ophthalmol. 2010;4:741-64. 2. Mocan MC, Uzunosmanoglu E, Kocabeyoglu S, Karakaya J, Irkec M. The association of chronic topical prostaglandin analog use with meibomian gland dysfunction. J Glaucoma. 2016;25(9):770-4. 3. Horsley MB, Kahook MY. Effects of prostaglandin analog therapy on the ocular surface of glaucoma patients. Clin Ophthalmol. 2009;3:291-5. 4. Shen W, Huang B, Yang J. Ocular surface changes in prostaglandin analogue-treated patients. J Ophthalmol. 2019;2019:9798272. 5. Cracknell KPB, Grierson I. Prostaglandin analogues in the anterior eye: their pressure lowering action and side effects. Exp Eye Res. 2009;88(4):786-91. 6. Arita R, Itoh K, Maeda S, et al. Effects of long-term topical anti-glaucoma medications on meibomian glands. Graefes Arch Clin Exp Ophthalmol. 2012;250(8):1181-5. 7. Park HYL, Kim JH, Lee KM, Park CK. Effect of prostaglandin analogues on tear proteomics and expression of cytokines and matrix metalloproteinases in the conjunctiva and cornea. Exp Eye Res. 2012;94(1):13-21. 8. Asiedu K, Abu SL. The impact of topical intraocular pressure lowering medications on the ocular surface of glaucoma patients: a review. J Curr Ophthalmol. 2018;31(1):8-15. 9. Zhang X, Vadoothker S, Munir WM, Saeedi O. Ocular surface disease and glaucoma medications: a clinical approach. Eye Contact Lens. 2019;45(1):11-8. 10. Zhou X, Zhang X, Zhou D, Zhao Y, Duan X. A narrative review of ocular surface disease related to anti-glaucomatous medications. Ophthalmol Ther. 2022;11(5):1681-704. 11. Parkkari M, Purola P, Uusitalo H. Ocular surface disease signs and symptoms of glaucoma patients and their relation to glaucoma medication in Finland. Eur J Ophthalmol. 2022;33(2):11206721221144339. 12. Lusthaus JA, Goldberg I. Brimonidine and brinzolamide for treating glaucoma and ocular hypertension; a safety evaluation. Expert Opin Drug Saf. 2017;16(9):1071-8. 13. Oh DJ, Chen JL, Vajaranant TS, Dikopf MS. Brimonidine tartrate for the treatment of glaucoma. Expert Opin Pharmacother. 2019;20(1):115-22. 14. Scozzafava A, Supuran CT. Glaucoma and the applications of carbonic anhydrase inhibitors. Subcell Biochem. 2014;75:349-59. 15. Supuran CT, Altamimi ASA, Carta F. Carbonic anhydrase inhibition and the management of glaucoma: a literature and patent review 2013-2019. Expert Opin Ther Pat. 2019;29(10):781-92. 16. Al-Humimat G, Marashdeh I, Daradkeh D, Kooner K. Investigational rho kinase inhibitors for the treatment of glaucoma. J Exp Pharmacol. 2021;13:197-212. 17. Saha BC, Kumari R, Kushumesh R, Ambasta A, Sinha BP. Status of rho kinase inhibitors in glaucoma therapeutics—an overview. Int Ophthalmol. 2022;42(1):281-94. 18. Wang J, Wang H, Dang Y. Rho-kinase inhibitors as emerging targets for glaucoma therapy. Ophthalmol Ther. October 14, 2023. [Epub ahead of print]. 19. Moshirfar M, Parker L, Birdsong OC, et al. Use of rho kinase inhibitors in ophthalmology: a review of the literature. Med Hypothesis Discov Innov Ophthalmol. 2018;7(3):101-11. 20. Amano M, Chihara K, Kimura K, et al. Formation of actin stress fibers and focal adhesions enhanced by rho-kinase. Science. 1997;275(5304):1308-11. 21. Raizman MB, Hamrah P, Holland EJ, et al. Drug-induced corneal epithelial changes. Surv Ophthalmol. 2017;62(3):286-301. 22. MacIver S, Stout N, Ricci O. New considerations for the clinical efficacy of old and new topical glaucoma medications. Clin Exp Optom. 2021;104(3):350-66. 23. Bhargava M, Sen S, Bhambhani V, Paul RS, Dutta C. Reticular epithelial corneal edema as a novel side-effect of rho kinase inhibitors: an Indian scenario. Indian J Ophthalmol. 2022;70(4):1163-70. 24. Lyons LJ, Wu KY, Baratz KH, Sit AJ. Honeycomb epithelial edema associated with rho kinase inhibition: a case series and review of the literature. Cornea. 2022;41(2):243-8. 25. Pflugfelder SC, Baudouin C. Challenges in the clinical measurement of ocular surface disease in glaucoma patients. Clin Ophthalmol. 2011;5:1575-83. 26. Kumar S, Singh T, Ichhpujani P, Vohra S. Ocular surface disease with BAK preserved travoprost and polyquaternium 1(Polyquad) preserved travoprost. Rom J Ophthalmol. 2019;63(3):249-56. 27. Skov AG, Rives AS, Freiberg J, et al. Comparative efficacy and safety of preserved versus preservative‐free beta‐blockers in patients with glaucoma or ocular hypertension: a systematic review. Acta Ophthalmol. 2022;100(3):253-61. 28. Saini M, Dhiman R, Dada T, Tandon R, Vanathi M. Topical cyclosporine to control ocular surface disease in patients with chronic glaucoma after long-term usage of topical ocular hypotensive medications. Eye (Lond). 2015;29(6):808-14. 29. Sherwin JC, Ratnarajan G, Elahi B, Bilkiewicz‐Pawelec A, Salmon JF. Effect of a punctal plug on ocular surface disease in patients using topical prostaglandin analogues: a randomized controlled trial. Clin Exp Ophthalmol. 2018;46(8):888-94. |
