 |
|
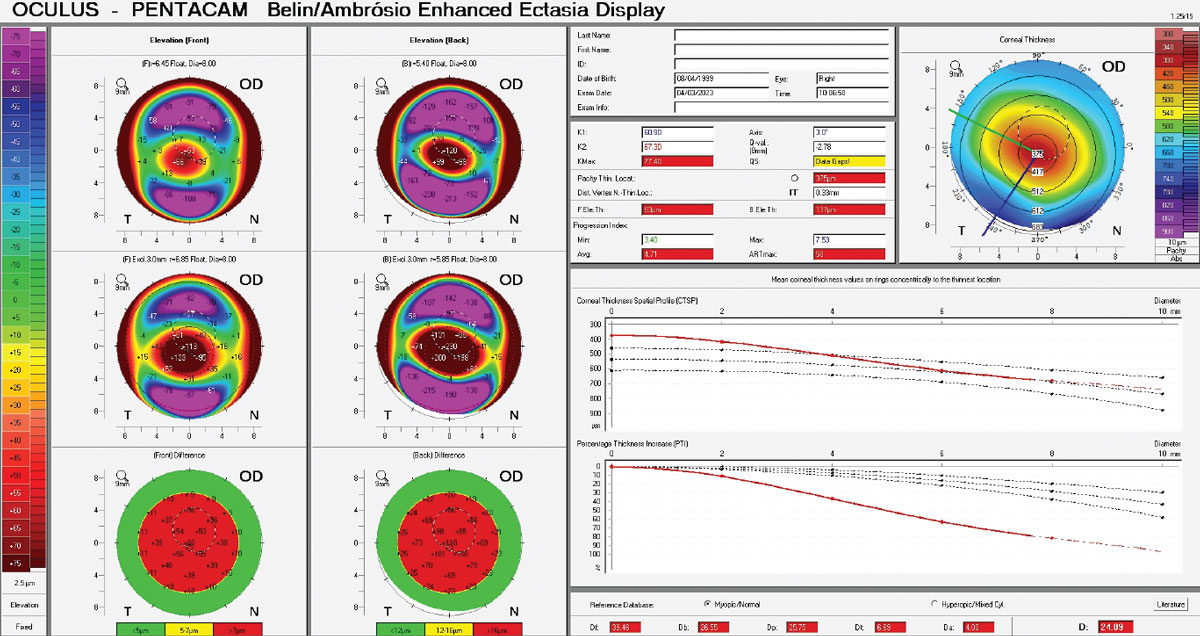
Study suggests patient stratification according to disease severity is essential not only when choosing cutoffs but also the variables to define KC progression. Photo: Christine Sindt, OD. Click image to enlarge. |
Cornea specialists within optometry and ophthalmology have made great strides in keratoconus (KC) care in the last decade, as the adoption of collagen crosslinking brought with it better visual outcomes, cost savings and a reduction in corneal transplants. However, the epidemiology of KC remains disputed and there is no consensus on how to establish progression of the disease among a variety of potential clinical metrics available. A recent study aimed to analyze how progression criteria classify a cohort of untreated KC and ascertain how this compares with previous clinical data.
This was a retrospective, longitudinal, observational study of 906 keratoconus patients. The criteria analyzed included keratometry (KMAX ), front astigmatism, pachymetry, the Belin ABCD progression display, front steep keratometry and mean radius of the back surface.
The study showed that using a single criterion to define KC progression (such as KMAX ) leads to excessively high rate of progressive cases unless the change is well over the repeatability threshold; however, combining two parameters to define progression, such as KMAX and front astigmatism, adds certainty to the decision when both are considered to be positive simultaneously.
“Ideally, the variables used should assess anterior and posterior surface steepening and/or corneal thinning, with a preference for repeatable, monotonic and consistent variables,” the researchers explained in their paper on the work. The authors noted that, in this context, zonal parameters generally outperform single-point variables such as KMAX or pachymetry. However, those same measures serve as a good combination to follow-up subclinical and very early KC, they said in their article, while the combination of front steep keratometry and mean radius of the back surface was their criterion of choice for the mild and moderate stages.
“KC is complex, and a one-fits-all definition of progression may not be the most appropriate approach,” they concluded. “Patient stratification according to disease severity is essential not only when choosing cutoffs but also the variables to define progression.”
Koppen C, Jimenez-Garcia M, Kreps EO, et al. Definitions for keratoconus progression and their impact on clinical practice. Eye & Contact Lens. July 29, 2023. [Epub ahead of print.] |
