| |
Volume 16, Number 1 |
March 2020 |
|
FROM
THE DESK OF THE EDITOR
Well, 2020 had been off to an interesting start to say the least. I never considered my job to be the work-from-home type, as I write this message from my living room couch with my kids, who are normally at daycare, playing on the floor. Now that the CDC has recommended postponing routine eye care, it puts many of us in an interesting postion. I am not an expert in public health or epidemiology, so I am listening and following the advice of the experts. All of us want to stay healthy to resume our normal as soon as possible.
We are charting unknown waters. But normal will eventually resume. Let’s try and keep our minds fresh in the meantime. I have a stack of journals on my desk that I have meant to read and many articles unread in my inbox. Until I can get back to normal patient care, that is my goal. Well, and also trying to stay sane at home with my children (whom I dearly love, but the lack of routine is driving us all crazy). So for now, I’ll leave you with an opportunity to get up to speed in retina.
Stay well!
Anna Bedwell, OD, FAAO
Editor-in-Chief
PRESIDENT'S MESSAGE
As I write this, fear and anxiety at near panic levels are rampant in our nation and around the world due to the spread of the coronavirus. Most of this fear comes from the unknown. Even the “experts” can’t answer all of the questions that unnerve the public, which leads to even greater anxiety. Fear of the unknown has been called the fundamental fear that fuels all other types of anxiety. At this time, all of the concerns surrounding this virus cannot be answered, but, from past experience, we do know that in time it will pass, and we can all return to normalcy.
As I have seen this fear grip many people, I have considered the fear that all of our patients experience when they are given a new diagnosis, especially one that has the possibility of taking their precious vision. This fear of the unknown regarding their vision is no less real than the fear that we see all around us right now. Through modern diagnostic testing, we can detect disease earlier intervene sooner, and, with modern treatments that weren’t even available a few short years ago, treat some of these diseases and prevent vision loss.
It is incumbent upon all of us as eye care providers to reduce the uncertainty of retinal and other ocular diseases as much as possible through patient education and, in turn, reduce the fear that our patients no doubt experience. Patients can have greater peace and calmness if they have enough information and will experience less fear of the unknown.
My best wishes are with each of you as we make our way through this current crisis. The one thing that I do know is that we will make it through and see much better days ahead.
Jeffrey Austin, OD, FAAO
ORS President

YOU
MAKE THE DIAGNOSIS
Answer appears later in newsletter.
Answer appears later in newsletter.
Image Gallery
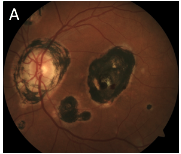
Which of the following images represents histoplasmosis scarring?
Answer appears later in the newsletter.
|
JOURNAL
ABSTRACTS
Collateral Vessels on Optical Coherence Tomography Angiography in Eyes with Branch Retinal Vein Occlusion
Collateral vessels form as a mechanism to reroute the drainage of blood from an occluded vein often times by crossing the horizontal raphe. OCTA appears superior to fluorescein angiongraphy (FA) in detecting collateral vessels. As such, this study sought to utilize OCTA to observe collateral formation in branch retinal vein occlusion (BRVO) and study the impact on macular edema.
This retrospective case series included patients with BRVO with macular edema that were examined by OCTA (baseline, three months, six months) +/- FA. All patients had at least six months of follow up. Treatment consisted of intravitreal ranibizumab and focal laser photocoagulation with panretinal photocoagulation if evidence of retinal neovascularization. On OCTA, collateral vessels were present in 23/28 eyes (82%) all evident at the baseline visit. All of the major BRVOs (18/18) had collaterals compared to 5/10 of the macular BRVOs. The eyes with collaterals had a greater mean baseline CRT (p=0.026) in contrast to those without collaterals. Furthermore, the eyes with collaterals responded faster to treatment with a greater CRT thickness reduction rate (p=0.014).
The authors concluded that collateral formation may develop earlier than previously thought since all of the patients with collaterals were present at baseline in the acute phase. Previous study has relied upon FA to observe collaterals. OCTA has an advantage over FA in its ability to visualize both the superficial and deep retinal layers. Further study is indicated to confirm these findings.
Suzuki N, Hirano Y, Tomiyasu T, et al. Collateral vessels on optical coherence tomography angiography in eyes with branch retinal vein occlusion. Br J Ophthalmol. 2019 Oct;103(10):1373-9.
Glaucoma after Iodine-125 Brachytherapy for Uveal Melanoma: Incidence and Risk Factors
Treatment of uveal melanoma with iodine-125 brachytherapy is generally preferred over the alternative of enucleation. However, radiation comes with the potential for a handful of ocular complications. This study looked specifically at the incidence of glaucoma, secondary open-angle and neovascular, after brachytherapy.
The retrospective case series included patients treated with brachytherapy for choroidal melanoma. A single surgeon at a tertiary care center performed all the procedures over a 10-year period. Glaucoma was defined by persistent elevated IOP readings with at least three readings ≥21 mmHg occurring over at least one month. Gonioscopy confirmed open angles and looked for presence of neovascularization. There were 374 eyes studied and of those, 31 (8.6%) developed open-angle glaucoma (OAG) over a median follow up of 2.14 years (range, eight days to 9.8 years). All but one, who needed drainage surgery, were treated with topical therapy. Secondary OAG was linked to increased age, higher baseline IOP, larger melanoma, melanomas involving the ciliary body and vitrectomy with silicone oil. Twenty-five eyes (6.7%) developed neovascular glaucoma over a median follow-up of 2.1 years. Neovascular glaucoma development was associated with larger melanoma, heavy smokers, pseudophakia and severe radiation retinopathy.
On Kaplan-Meier curve, the five-year estimated incidence was 15% for OAG and 13% for neovascular glaucoma. This study boasted a large number of patients and long follow-up period. As glaucoma diagnosis was made on the basis of IOP, rather than looking at optic nerve structure and function, the study may under account for some cases of OAG. Given these high incidence findings, patients treated with iodine-125 brachytherapy should be carefully monitored for glaucoma and neovascularization.
Kim EA, Salazar D, McCannel CA, et al. Glaucoma after iodine-125 brachytherapy for uveal melanoma: Incidence and Risk Factors. J Glaucoma. 2020 Jan:29(1):1-10.
Clinical Effectiveness of Intravitreal Therapy with Ranibizumab vs. Aflibercept vs. Bevacizumab for Macular Edema Secondary to Central Retinal Vein Occlusion: A Randomized Clinical Trial
The treatment for macular edema from central retinal vein occlusion (CRVO) consists of anti-VEGF injections. But what agent to choose? The clinical effectiveness must be considered as well as the cost for the patient and healthcare system. The LEAVO (Lucentis, Eylea, Avastin in Vein Occlusion) study compared the commonly used options of ranibizumab, aflibercept and bevacizumab in a randomized, prospective, noninferiority trial. Noninferiority was defined as above -5 LogMAR letters.
The trial consisted of 463 eyes with macular edema from CRVO recruiting patients across 44 hospitals in the United Kingdom. Change in BCVA at 100 weeks was the primary endpoint. At completion, the gain in acuity letters was 12.5 for ranibizumab, 15.1 for aflibercept and 9.8 for bevacizumab. The central thickness by OCT decreased by 405 µm for ranibizumab, 378 µm for aflibercept and 334 µm for bevacizumab. Aflibercept performed better in terms of number of injections at a mean of 10 injections compared with ranibizumab and bevacizumab at 11.8 and 11.5 injections, respectively. The authors concluded that aflibercept was noninferior (no worse than) to ranibizumab, while bevacizumab was not noninferior to ranibizumab treatment.
Over the course of two years, all three anti-VEGF agents showed improved and sustained BCVAs. The lowest cost option, bevacizumab, was effective, but not on the same level as ranibizumab and aflibercept. The researchers found a lower number of mean injections of aflibercept. This may be particularly noteworthy considering that some patients require treatment spanning over years.
Hykin P, Prevost AT, Vasconcelos JC, et al (LEAVO Study Group). Clinical effectiveness of intravitreal therapy with ranibizumab vs aflibercept vs bevacizumab for macular edema secondary to central retinal vein occlusion: a randomized clinical trial. JAMA Ophthalmol. 2019; Aug 29. [Epub ahead of print].
Bariatric Surgery Might Aggravate Proliferative Diabetic Retinopathy
Bariatric surgery (BS) has been proven as an effective treatment to help facilitate weight loss and rapid glycemic control in those with type 2 diabetes. In fact, up to 80% of patients that undergo BS have a remission in type 2 diabetes within two years. Multiple studies have assessed the effect of BS on diabetic retinopathy with widely varying results. The purpose of this study was to assess how BS affects patients with proliferative diabetic retinopathy (PDR) and compared 37 eyes with PDR who underwent BS to 37 eyes with PDR who did not.
The patients had to have at least one pre-op retinal examination and one post-op retinal examination at one year. This study found that the BS group had significantly higher incidence of intraocular hemorrhages, neovascular glaucoma and retinal vein occlusions than the control group at one year. In fact, 80.9% of patients from the BS group experienced ocular complications, as opposed to only 11.1% in the control group.
Additionally, researchers found that many of the patients from the BS group discontinued their ophthalmology visits during the first six months after surgery. However, both groups had similar, statistically significant visual acuity loss at one year.
Limitations of this study included small sample size, short follow-up time and treating fellow eyes of patients as independent in statistical analyses. Regardless, researchers wrote, it is important to follow diabetic patients closely in the months following BS to monitor for changes in retinopathy and to reiterate the importance of continued follow-up even though many patients may come off their systemic medications.
Sever O, Horozoglu F. Bariatric surgery might aggravate proliferative diabetic retinopathy. Acta Ophthalmol. 2020; Jan 7. [Epub ahead of print].
Intraocular Pressure Change after Injection of Intravitreal Dexamethasone (Ozurdex) Implant in Korean Patients
Dexamethasone (DEX) intravitreal implant (Ozurdex) was approved in 2009 for the treatment of macular edema. It has been shown to improve visual acuity and reduce central retinal thickness on optical coherence tomography, with an added benefit of delivering treatment over an extended time with just one injection. However, multiple studies have shown an increase in IOP as an adverse event, although most of these studies have focused on subjects of Western descent. This study analyzed the IOP changes after a DEX implant for macula edema over one year in Korean patients.
A total of 540 eyes were included, and the primary causes of macular edema were BRVO and DME, followed by CRVO and then uveitis. Investigators found that IOP gradually increased until two months post-injection and then gradually decreased back to baseline at 12 months. The overall incidence rate of IOP elevation after DEX implant was 12.6%, and it differed between those without glaucoma and those with glaucoma using an IOP-lowering medication, with an incidence of 9.6% and 38.8%, respectively.
Overall, only 10.9% of eyes with elevated IOP needed to add an IOP-lowering medication. This study concluded that the incidence of eyes with an IOP elevation after DEX implant was much lower than other large, randomized studies such as the MEAD, GENEVA and HURON studies, and the increase in IOP was also lower at almost all measured time points. Additionally, the number of eyes that needed an additional IOP-lower medication was much lower than most Western-based studies. This suggested that intravitreal DEX injection could be a safe treatment option for Asian patients with macular edema.
Choi W, Park SE, Kang HG, et al. Intraocular pressure change after injection of intravitreal dexamethasone (Ozurdex) implant in Korean patients. Br J Ophthalmol. 2019;103:1380-7.
Predictors of Enucleation in Coats Disease: Analysis of 259 Eyes of 259 Patients at a Single Center
Coats’ disease is a non-hereditary, unilateral retinal vascular disease, usually affecting males in the first decade of life. Patients present with telangiectatic vessels, micro and macroaneurysms, and intraretinal and subretinal exudation. This was a retrospective study of patients with Coats’ disease seen in Ocular Oncology of the Wills Eye Hospital.
The study included 259 patients and 32 (12%) of those eyes required enucleation. Indications for enucleation included neovascular glaucoma (75%), concern for intraocular tumor (19%) and phthisis bulbi (6%). Eyes that had to be enucleated presented with far more advanced disease, including neovascular glaucoma, total retinal detachment, and greater telangiectatic vessels, aneurysms and subretinal fluid. In fact, an increase in subretinal fluid on ultrasonography increased the risk for enucleation by 20%, and each additional clock hour of aneurysms on angiography by 35%.
Interestingly, 53% of the enucleation group had enucleation as the first form of treatment. However, because the study site was an ocular oncology center, many of the patients had been referred for retinoblastoma and already had advanced disease. Also of note, the study spanned over four decades, and fewer cases each decade were managed with enucleation, likely because of more advanced imaging modalities and superior treatment options.
The authors concluded that it is important to diagnose patients with Coats’ disease as early as possible so better treatment options can be employed and enucleation can be avoided.
Udyaver S, Dalvin LA, Lim LS, et al. Predictors of enucleation in Coats disease: analysis of 259 eyes of 259 patients at a single center. J AAPOS. 2019; 23:266.e1-9.
|
ANSWER
TO "YOU MAKE THE DIAGNOSIS"
An intraocular malignant neoplasm is one of the most feared diagnosis to convey to a patient. The visual prognosis is usually poor, and the potential for systemic involvement is worrisome. Making the correct assessment before sending the patient out for further testing is imperative, as other disorders can masquerade as a malignancy. Such is the case with the condition below where only five percent of practitioners referred the patient with the correct diagnosis.1
The Patient
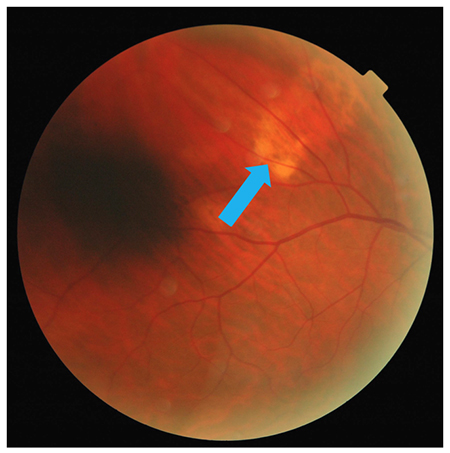
A 69 year-old Caucasian male presented for follow up of mild stage primary open-angle glaucoma, age-related nuclear cataracts and an area of retinal pigment epithelium (RPE) dropout superiorly OD. His medical history included type 2 diabetes, essential hypertension, hyperlipidemia, coronary artery disease, congestive heart failure, benign prostatic hyperplasia and obstructive sleep apnea. Systemic and ocular medications included atorvastatin, carvedilol, insulin, latanoprost, losartan, metformin and tamsulosin. Social history was positive for smoking (half-pack per day) and recreational drugs (marijuana).
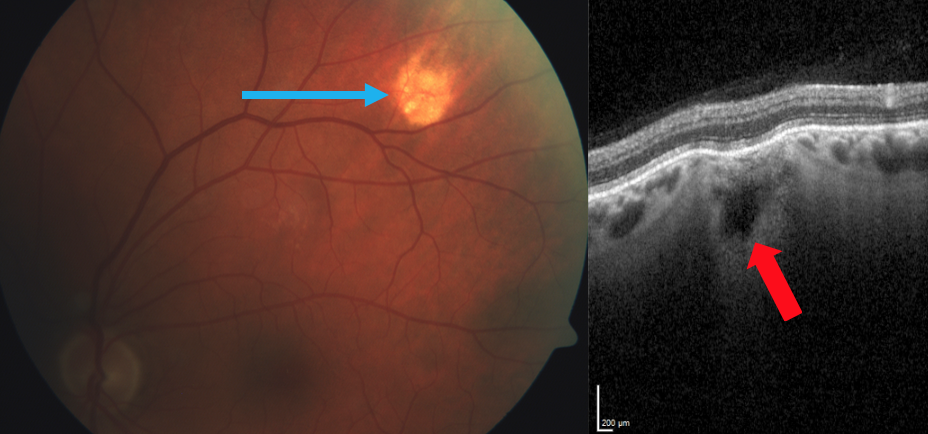
Best-correct visual acuities were 20/20 OD, OS with +0.75-0.50 x 120 OD and +0.25-0.50 x 115 OS and a +2.50 add. Chair skills were unremarkable. Slit-lamp biomicroscopy showed a pinguecula OU and NC2 OU as graded by the lens opacities classification system (LOCS) III. A dilated fundus examination revealed a cup-to-disk ratio of 0.70V/0.65H OD and 0.50 OS, along with a yellow, subretinal lesion outside the superior temporal arcade (Figure 1, see above).
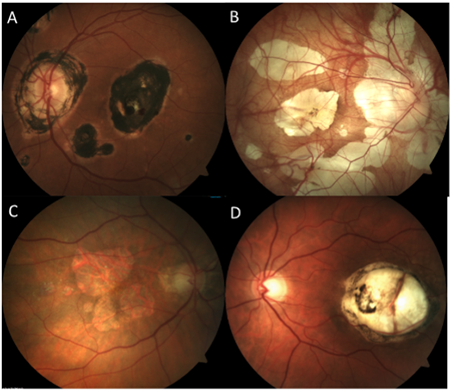
Enhanced-depth imaging optical coherence tomography (EDI-OCT) through the area demonstrated choroidal thinning above the lesion (Figure 2, see below). B-scan ultrasonography highlighted an echo-dense placoid mass with acoustic orbital shadowing (Figure 3, see below).
Discussion and Follow Up
Sclerochoroidal calcification (SCC) is a deposition of calcium within the sclera. They present as single or multiple, round focal lesions along the superior temporal arcades most commonly seen in the elderly as an incidental finding.2–4 SCCs appear pale yellow, white or orange, and can be flat or up to 6mm in height.5 Shields, et al. analyzed 179 eyes of 118 patients with SCC and found the vast majority to occur in Caucasians (98%) with a mean age of 69 (32 to 95 range) and a 60:40 female-to-male ratio.1 Laterality approached 50% for all categories: unilateral vs. bilateral, and right eye vs. left eye.1
The term SCC is actually a misnomer, as the calcification represents a scleral mass. There are four recognized types: Type 1 “flat,” Type 2 “rolling,” Type 3 “rocky-rolling” and Type 4 “table mountain.”6 “Rocky-rolling” (Figure 4, see below) represents the most common type and causes the most thinning of the overlying choroid, which in turn leads to a greater possibility for adjacent retinal pigment epithelium (RPE) and outer retinal changes.6 The hill-like elevation in this patient (Figure 2, see below) characterizes a Type 2 “rolling” SCC.
Differentiating SC from more insidious lesions is key to preventing superfluous testing. Fundoscopy alone can diagnose SCC given its characteristic appearance, demographic and predilection for the superior temporal location. With EDI-OCT, an SCC will appear as a scleral (not choroidal) plaque with secondary compression of the choroid.3,7 B-scan ultrasonography shows a highly reflective, echo-dense plaque unlike a choroidal metastasis, which would likely exhibit low- to -medium reflectivity. The majority of SCCs exhibit homogeneous hyperautofluorescence with fundus autofluorescence (FAF) and hyperreflectivity on infrared (IR) imaging.7 SCCs also lack vasculature on a fluorescein or indocyanine green angiography. On computed tomography (CT) scans, SCCs appear as highly attenuated objects similar to bone. The CT scan easily confirmed the right eye SCC in this patient, and surprisingly picked up a subtle one in the left eye which was not viewed clinically (Figure 5, see below). This likely represents a Type 1 “flat” lesion, which is detectable only with ultrasonography or CT exam.1
Approximately 80% of SCCs are primary or idiopathic.1,6 Secondary causes result from hypercalcemia due to hyperparathyroidism, parathyroid adenomas, hypervitaminosis D, calcium pyrophosphate dihydrate deposition (CPPD), hypomagnesemia, diuretic use, chronic kidney disease and rarely renal disorders including Bartter’s syndrome.2,5,8
Patients with hyperparathyroidism display the mnemonic “stones, bones, groans, thrones and psychiatric overtones” due to kidney stones, bone pain, abdominal pain, polyuria and psychiatric symptoms such as depression, anxiety, insomnia, cognitive dysfunction and possibly coma.9
Bartter’s syndrome represents a group of inherited primary renal tubular electrolyte transport disorders. Of the three phenotypes, only two – classic Bartter’s and Gitelman’s – have been associated with SCC.8 Both of these closely related autosomal recessive diseases share the characteristics of renal salt wasting and hypokalemic hypochloremic metabolic alkalosis.10 A manifestation of Gitelman’s syndrome – which is more common and presents later in childhood or adulthood – includes hypomagnesemia.11 Magnesium ions increase CPPD crystal solubility. Therefore, hypomagnesemia could lead to deposition of those calcium crystals in joints and the sclera.11
SCCs are usually a benign finding. Similar to a Cogan or senile scleral calcified plaque which occurs near the horizontal rectus muscle insertions, some speculate that SCCs may be their counterparts at the oblique muscle insertions where chronic forces induce both primary and secondary calcifications.5 Rarely, SCCs may lead to a secondary choroidal neovascular membrane (CNV). Therefore, periodic monitoring with a dilated exam and EDI-OCT is recommended.2,9 If a CNV presents, some suggest observation may be the best initial course of action given the more peripheral location to the macula.12 Intravitreal anti-vascular endothelial growth factor (VEGF) injections or argon laser prove successful when utilized.12 Another unusual complication involved a case with a significant hyperopic shift and Adie’s tonic pupil.13 The authors cited damage to the postganglionic parasympathetic fibers, which travel in the suprachoroidal space on their way to the iris sphincter as the cause for the pupil abnormality.13
Conclusion
SCCs can impersonate various intraocular tumors and are frequently misdiagnosed.2,5,9 Typically, they represent an idiopathic incidental finding, but their discovery does warrant appropriate systemic testing to rule out underlying conditions. This may include a complete metabolic panel (CMP), parathyroid and renal function tests.7 Medications should also be reviewed as diuretics can lead to a loss of metabolic parameters.1 More importantly, however, is making the right diagnosis and avoiding unnecessary testing.
Jim Williamson, OD, FAAO, FORS
Abbey Kirk, OD
*Case also featured in upcoming Review of Optometry
 |
| Figure 2. EDI-OCT through the SCC reveals a Type 2 “rolling” lesion. Note the choroidal thinning at the above the lesion (red arrow). |
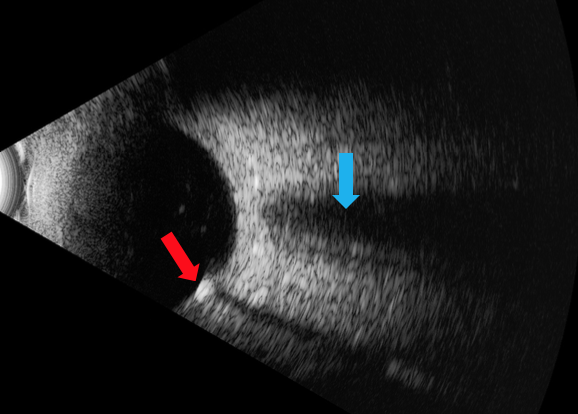 |
| Figure 3. B scan ultrasound using the 10MHz probe highlights the echo-dense placoid lesion (red arrow) with acoustic orbital shadowing which appears much smaller than – but similar to – the optic nerve, which is shown above this area (blue arrow). |
 |
| Figure 4. A Type 3 “rocky-rolling” appearance in another patient with SCC. Note the extensive choroidal thinning above the scleral mass (red arrow). |
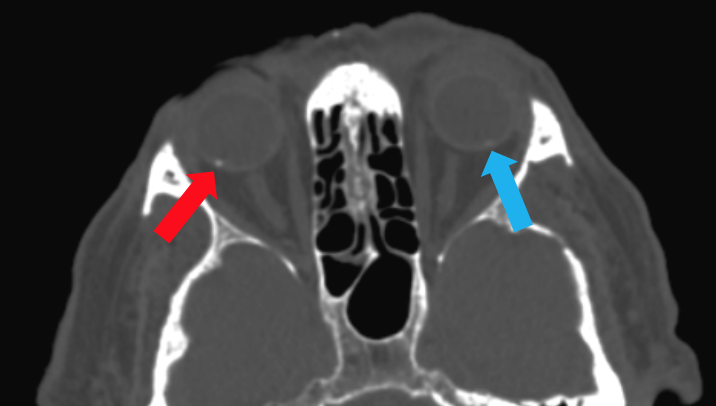 |
| Figure 5. Computed tomography (CT) scan demonstrates a SCC in the right eye (blue arrow) and a subtle one in the left eye, which was not visible on clinical exam. |
1. Shields CL, Hasanreisoglu M, Saktanasate J, Shields PW, Seibel IR a, Shields J a. Sclerochroidal calcification: Clinical features, outcomes, and relationship with hypercalcemia and parathyroid adenoma in 179 eyes. Retina. 2015;35:547-554.
2. Ali ZC, David VP. Sclerochoroidal calcification associated with hypovitaminosis D. Can J Ophthalmol. 2017;52(4):e121-e122.
3. Honavar SG, Shields CL, Demirci H, Shields JA. Sclerochoroidal calcification: Clinical manifestations and systemic associations. Arch Ophthalmol. 2001;119:833-840.
4. Leys A, Stalmans P, Blanckaert J. Sclerochoroidal calcification with choroidal neovascularization. Arch Ophthalmol. 2000;118:854-857.
5. Wong CM, Kawasaki BS. Idiopathic sclerochoroidal calcification. Optom Vis Sci. 2014;91(2):32-37.
6. Hasanreisoglu M, Saktanasate J, Shields PW, Shields CL. Classification of sclerochoroidal calcification based on enhanced depth imaging optical coherence tomography “mountain-like” features. Retina. 2015;35:1407-1414.
7. Fung AT, Arias JD, Shields CL, Shields JA. Sclerochoroidal calcification is primarily a scleral condition based on enhanced depth imaging optical coherence tomography. JAMA Ophthalmol. 2013;131(7):960-963.
8. Goerlitz-Jessen M, Ali MH, Grewal DS. Rare complications of sclerochoroidal calcifications. JAMA Ophthalmol. 2019;137(1):111-112.
9. Sugarman J, Douglass A, Say EA, Shields C. Stones, bones, groans, thrones, and psychiatric overtones: Systemic associations of sclerochoroidal calcification. Oman J Ophthalmol. 2017;10(1):47-49.
10. Fulchiero R, Seo-Mayer P. Bartter Syndrome and Gitelman Syndrome. Pediatr Clin North Am. 2019;66(1):121-134.
11. Bourcier T, Blain P, Massin P, Grünfeld JP, Gaudric A. Sclerochoroidal calcification associated with Gitelman syndrome. Am J Ophthalmol. 1999;128(6):767-768.
12. Bessette AP, Singh AD. Multimodal imaging of choroidal neovascularization associated with sclerochoroidal calcification. Ocul Oncol Pathol. 2016;2(4):234-238.
13. Zhang J, Davis AS, Spitze A, Lee AG. Bilateral adie’s tonic pupil and hyperopic shift in idiopathic sclerochoroidal calcification. Neuro-Ophthalmology. 2015;39(2):96-99.
|
IN THE
NEWS
 |
Genetic Testing for Free?
Sometimes you really can get something for nothing. Invitae and Blueprint Genetics are currently offering no-cost genetic testing for patients.
Through its ID Your IRD® program, Invitae offers its services for patients suspected of having an inherited retinal disease (IRD) and who have experienced one or more of the following symptoms: peripheral field loss, nyctalopia, color vision changes, central vision loss or photophobia. Of note, the program is not appropriate for age-related macular degeneration or ocular/oculocutaneous albinism. The test covers about 250 genes, and providers can expect results within 10 to 21 calendar days.
The Blueprint Genetics version – My Retinal Tracker Program – is for patients in the United States with IRD. The panels cover 322 genes targeting ones associated with IRD. To provide this service, the Foundation for Fighting blindness partnered with Blueprint Genetics and InformedDNA®. Upon receipt of the sample, clinicians can expect a turnaround time of about four weeks.
Both programs offer patients no-charge genetic counseling to help them understand their results.
|
|
Illuminated Scleral Indentor Enters the Market
Combining indenting and peripheral transscleral illumination, the ViPer (a portmanteau for “visible” and “periphery”) provides surgeons enhanced views of the retinal periphery and allows them to work autonomously without requiring additional personnel. The ViPer is a rounded, semi-transparent device that attaches to the endo illuminator and fits between the speculum and the scleral surface. The 360-degree ensures easy application and excellent mobility, according the Oertli®, the product’s maker.
|
|
First-Ever Treatment for Thyroid Eye Disease Gets FDA Nod
Finally, a non-surgical option for a thyroid eye disease (TED). Tepezza® (teprotumumab-trbw) is a fully human monoclonal antibody (mAb) and a targeted inhibitor of the insulin-like growth factor 1 receptor (IGF-1R) for the treatment of active TED. Delivery of the drug occurs through an intravenous (IV) infusion once every three weeks for a total of eight sessions – each one lasting up to 90 minutes. After six months, between about 70 to 80% of treated patients vs. 10 to 20% in the placebo group in two studies demonstrated a greater than 2mm reduction in proptosis. The majority of patients (86%) were Caucasian, followed by African American (8%), Asian (4%) and all others (2%). Side effects include inflammatory bowel disease (IBD) exacerbation and increased blood sugar. Estimated costs are around $15,000 per vial and about $200,000.
|
|
Device Detects Minuscule Eye Movements, Aims for Neurological Assessment
To evaluate neurological health such as concussions, providers may employ eye movement tests such as the King-Devick Test. A California-based company now says it has a device that detects movements as small as 1/100th the width of a human hair.
The C. Light system is based on a Tracking Scanning Laser Ophthalmoscope (TSLO) and is reportedly 120 times more sensitive than traditional technologies. Results of the 10-second test are then put through artificial intelligence-based algorithms to see if a possible match occurs with that of a known neurological disorder. The initial plan is to assess and track multiple sclerosis (MS), and later other disorders such as Alzheimer’s and Parkinson’s.
|
|
Usher Syndrome Type 2 and Non-Syndromic Retinitis Pigmentosa Patients See Hope
ProQR® Therapeutics received Rare Pediatric Disease Designation (RPD) from the FDA for QR-421a – a first-in-class investigational RNA-based oligonucleotide designed to address the underlying cause of vision loss in Usher syndrome type 2 and non-syndromic retinitis pigmentosa due to mutations in exon 13 of the USH2A gene. Given by intravitreal injection, QR421a is designed to restore functional Usherin protein by using an exon skipping approach with the aim to stop or reverse vision loss in patients. The company has another drug – sepofarsen (QR-110) – which is currently in Phase 2/3 study for Leber’s congenital amaurosis.
|
|
A “Cheap” OCT?
Duke University biomedical engineers recently developed a low-cost portable OCT, which produces images comparable to available commercial systems. The device features a 3D-printed spectrometer that costs 1/10th the price of current retail units.
The new type of spectrometer takes the light on a circular path within a 3D-printed plastic, which keeps the optical elements aligned. Misalignments are minimized by the use of a large detector. Estimated cost is $15,000.
|
|
Clinical Trials Tests Safety of Novel Potential Treatment for Geographical Age-Related Macular Degeneration
Researchers at the National Eye Institute (NEI) launched the first clinical trial of patient-derived stem cell therapy to replace retinal pigment epithelial (RPE) cells in geographical age-related macular degeneration (AMD). Blood cells derived from the patient are converted to induced pluripotent stem cells (iPSC), which have the potential to form any cell type. Researchers then program the iPSC to become RPE cells. A specifically designed device then inserts the one-cell-thick monolayer between the RPE and photoreceptors. The goal is to protect the remaining photoreceptors.
|
|
Diabetes Educator Group and Association Transition to New Name
To better align their professional designation and duties, the credential Certified Diabetes Educator (CDE) will now be referred to as Certified Diabetes Care and Education Specialist (CDES). Also, the American Association of Diabetes Educators (AADE) changed its name to Association of Diabetes Care & Education Specialists (ADCES).
Why the change? The group’s leaders felt their responsibilities included much more than just education. They work in a variety of settings such as hospitals, doctor offices and public health centers.
Eyecare providers may want to consider the services of this group, given it is covered by Medicare and most private insurers. Unfortunately, according to the CDC, of those with diabetes, less than 5% of Medicare beneficiaries and 7% of privately insured people participate in the program within the first year of diagnosis.
|
| |
| |
|
|
IMAGE QUIZ ANSWER
The correct answer, image A, demonstrates scarring from presumed ocular histoplasmosis syndrome (POHS). POHS is caused by exposure to fungus spores (Histoplasma capsulatum). This produces a generally asymptomatic infection in the lungs that presumably travels to the eye via the bloodstream. The risk for exposure to histoplasmosis is higher for those living near the Ohio and Mississippi River Valleys where the fungus is present in the soil. Retinal findings of POHS include chorioretinal scars, termed “histo spots,” and peripapillary atrophy. After the initial infection, eyes with POHS carry a risk of developing choroidal neovascular membranes.
B: pathological myopia
C: geographic AMD
D: toxoplasmosis
|
WHY BECOME AN ORS FELLOW?
By Bill Denton, O.D., F.A.A.O.
Chair, Membership Committee
At some point in your career, you realize you just may be coasting. Your knowledge has been limited to the journals you receive and attempt to read, and the conferences that may not be as fulfilling as they once were. You simply need a challenge that will add an extra dimension to your professional learning.
Fellowship in the Optometric Retina Society (ORS) can provide several benefits in addition to the initial challenge of qualifying for this honor. Plenty of perks accompany your induction, but the coolest part is being associated with a body of knowledge and resources which can help you in many other ways. It is not uncommon to receive weekly thought-provoking emails about challenging cases and treatment dilemmas. Some fellows like to share their awesome cases they have diagnosed, while others post their cases with hopes that other Fellows will suggest an alternative differential diagnosis. At times it is like a round-table of brainstorming, but through the use of modern technology. Fellowship has little obligation with a huge opportunity for professional growth.
If you are up to the challenge of becoming a Fellow of the ORS, feel free to peruse the details and application at www.optometricretinasociety.org. Advice can be given to assist you in your quest. Feel free to contact us.
|

Editor
in Chief
Anna K. Bedwell, OD, FAAO
Co-Editor
Brad Sutton, OD, FAAO |
Journal
Reviewers
Larissa Krenk, OD
Contributor
Jim Williamson, OD, FAAO
Senior Graphic Designer
Matt Egger
|
Review of Optometry® is published by the Review Group, a Division of Jobson Medical Information LLC (JMI), 11 Campus Boulevard, Newtown Square, PA 19073.
To subscribe to other JMI newsletters or to manage your subscription, click here.
To change your email address, reply to this email. Write "change of address" in the subject line. Make sure to provide us with your old and new address.
To ensure delivery, please be sure to add revoptom@lists.jobsonmail.com to your address book or safe senders list.
Click here if you do not want to receive future emails from Review of Optometry. |
|