 |
| Click image to enlarge. |
Good as it is, the standard CXL protocol has been limited to a stromal thickness of more than 400μm, depriving many needy patients of the valuable procedure. However, new research suggests an updated method using individualized fluence could expand CXL treatment to ultra-thin corneas. The new method, referred to as “sub400,” uses lower fluence to modulate penetration depth. The study, published in the American Journal of Ophthalmology, reported promising results, with the sub400 technique stopping keratoconus progression about 90% of the time over 12 months.
The standard crosslinking “Dresden” protocol combines 3mW/cm2 UV intensity for 30 minutes, for a total UV delivery (or “fluence”) of 5.4 J/cm2. Limited to corneas with a stromal thickness of more than 400μm, the Dresden Protocol cross-links approximately the first 330µm of the cornea, leaving a 70µm safety margin for the corneal endothelial cells, but corneas with advanced keratoconus often fall below this threshold and require the use of modified protocols, all of which go along with major drawbacks, explains researcher Farhad Hafezi, MD, PhD.
The sub400 protocol simplifies things and helps avoid the variability in effect introduced by contact lenses and swelling the cornea, Dr. Hafezi adds.
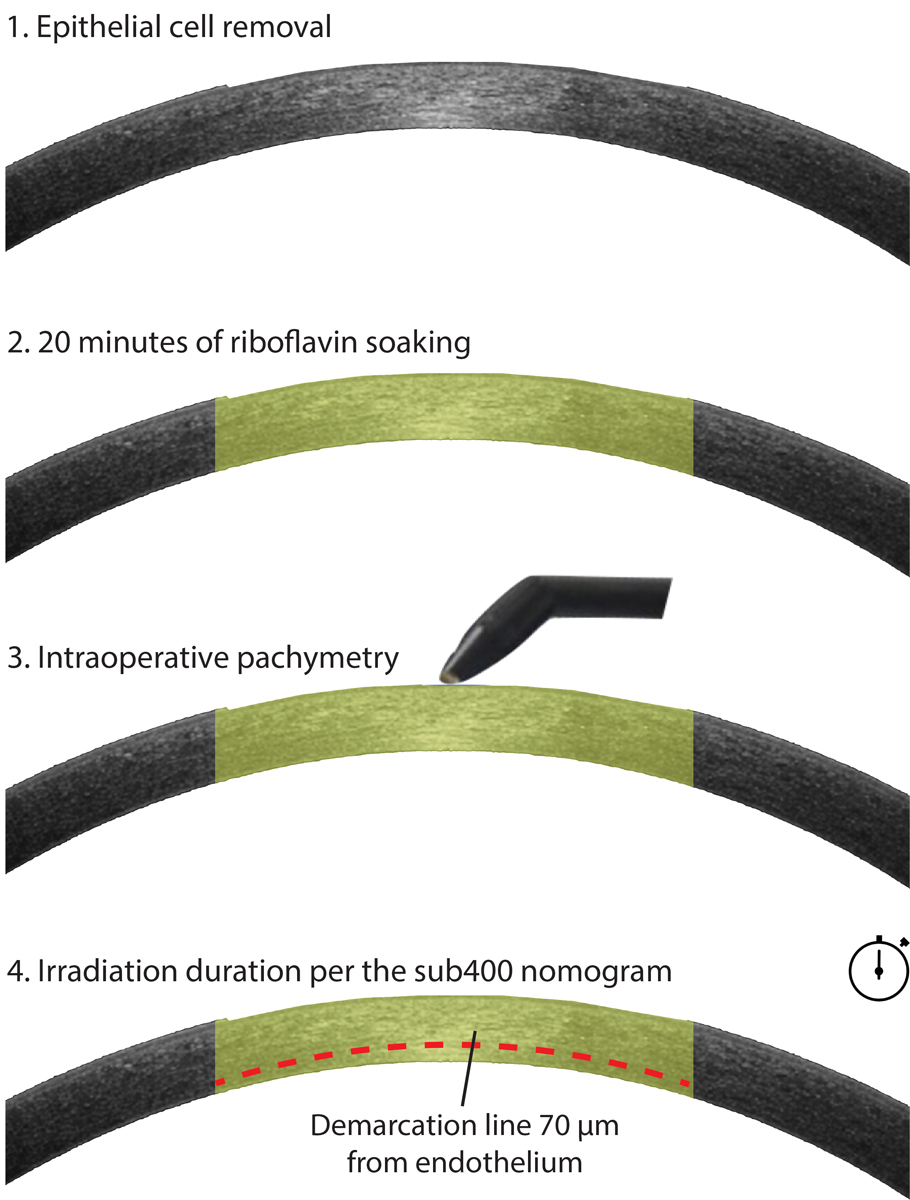
The sub400 protocol involves measuring corneal thickness after riboflavin application, just prior to irradiation, then calculating a total UV fluence based on the patient’s individual thickness.
The success rate of the sub400 protocol is 89% and, since a base intensity of 3mW/cm2 is used, it can be performed with any existing CXL technology in corneas that would otherwise have required corneal transplantation, Dr. Hafezi says.
His team’s retrospective, interventional case series included 39 eyes with progressive keratoconus and corneal stromal thicknesses between 214µm and 398μm at the time of UV-irradiation. After epithelium removal, UV-irradiation was performed at 3mW/cm2 with the length of exposure depending on the stromal thickness. Participants underwent exams prior to surgery and up to 12 months after the procedure.
After sub400, 35 eyes (90%) achieved tomographical stability at one year, with no eyes showing signs of endothelial decompensation. The researchers observed a significant correlation between stromal demarcation line depth and irradiation time, but not between stromal demarcation line depth and change in the maximum keratometry value. On average, the study reported a significant change in the thinnest stromal thickness (-14.5μm), maximum keratometry value (-2.06D) and densitometry (+2.00 grayscale units), but no significant changes corrected distance visual acuity, sphere or cylinder.
Since the demarcation line depth didn’t predict treatment outcome, the researchers suggested depth is unlikely related to the extent of CXL-induced corneal stiffness, but rather to the extent of CXL-induced microstructural changes and wound healing.
| Hafezi F, Kling S, Gilardoni F, et al. Corneal crosslinking with riboflavin and UVA in ultra-thin corneas: the sub400 protocol. Am J Ophthalmol. December 16, 2020. [Epub ahead of print]. |