Oral medications play a very important and clearly defined role in daily practice. Our profession has grown and matured significantly during the last three decades, and now the vast majority of us are able to prescribe more orals than ever before. Expanded prescribing rights allow us to more effectively manage our patients, as well as bring additional value and savings to the health care system.
Although several categories of oral medications play an important role in patient care, anti-infectives and analgesics are among the most frequently prescribed agents. In order to effectively use these medications in clinical practice, however, it is essential to balance a number of factors—such as side effect profiles, drug allergies and pregnancy status—that will ultimately lead to the success or failure of treatment.
|
|
|
|
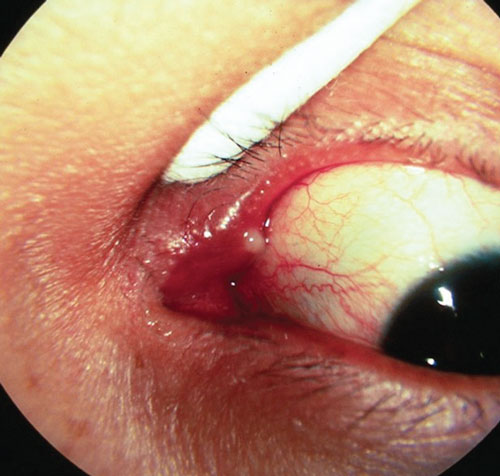
Which oral antibiotic would be most appropriate to treat dacryocystitis, as seen in this patient? |
A Lesson in History
Before initiating oral meds, a complete ocular and systemic history is crucial. This includes detailed knowledge of any other medications the patient is taking and whether the individual has any relevant drug allergies. Also, it is important document his or her general health status—particularly liver and kidney function. Remember that proper liver function is critical for the metabolism of oral medications, and kidney function is integral to drug excretion.
A practical pointer—when encountering patients with extensive medication lists and multiple drug allergies, it may be helpful to ask them which agents they’ve used in the past for pain management or certain infections. We have several of these patients in our practice. Over time, many of them have learned which pain medications, for example, they can take without difficulty.
Oral Anti-Infective Agents in Eye Care
We like to employ the “big bottle theory” when prescribing oral medications. If you look behind the counter in any pharmacy, you will see all sizes and shapes of pill bottles. The understood rule here is that the medications kept in the biggest bottles are the ones that are most often used, so the pharmacy keeps more of them on hand. Although there certainly are times when less common medications are needed, it is our experience that most infectious ocular conditions can be treated with five to six oral agents.
Determining whether the infectious process at hand is acute or chronic is the first decision point in our medication selection process. Once we have made this determination, we then go to our “Fabulous Five” oral anti-infectives to select the most appropriate drug for that individual.
Our ‘Fabulous Five’ Oral Antibiotics
1. Amoxicillin
with or without clavulanic acid. This is a great choice for soft tissue infections, such as hordeolum, preseptal cellulitis, dacryocystitis and dacryoadenitis.1
Amoxicillin is a member of the penicillin family. It does not kill bacteria directly, but prevents them from multiplying by prohibiting cell wall formation. When clavulanic acid is added to amoxicillin, it enhances the agent’s bactericidal effect via inactivation of the enzyme beta lactamase. This further prohibits microbial resistance against organisms that produce beta lactamase, such as S.aureus
, S.epidermidis
and H.influenza.2

|
|
| In addition to amoxicillin, which oral anti-infective agent demonstrates good clinical efficacy against preseptal cellulitis, as seen here? |
|
Anyone with children knows that pediatricians prescibe amoxicillin and Augmentin (amoxicillin/clavulanic acid, GlaxoSmithKline) for a variety of infections. Augmentin is especially good against gram-negative H.influenza.2 It is available in a variety of formulations and flavors, and is our first choice in children with acute infections.
Specifically for use in pediatric patients, Augmentin is prescribed as 20mg/kg/day to 40mg/kg/day for no more than 10 days. Any time we treat children, we always call their pediatrician as a courtesy and send a follow-up letter. This has proven to be a great practice builder, frequently resulting in referrals.
For adults, dosing should be 500mg to 875mg BID for five to seven days. Further, because Augmentin is a Category B drug, it can be used by female patients who are pregnant or nursing.
If Augmentin is prescribed, it should be taken with food or milk to improve clavulanic acid absorption. Be sure to document hepatic function in the patient history, because the drug is contraindicated in those with acute liver injury and/or liver disease.
2. Cephalexin. For adults with soft tissue infections (e.g., preseptal cellulitis, dacryocystitis, dacryoadenitis), our first choice is Keflex (cephalexin, Advancis Pharmaceutical) at a dosage of 250mg to 500 mg QID for 10 to 14 days. Cephalexin is a member of the cephalosporin antibiotic class. These agents demonstrate a similar mode of action and side effect profile as the penicillins.
Keflex is a great choice due to cost and proven efficacy. Although Augmentin would be our first choice for pediatric patients, Keflex can also be dosed at 25mg/kg/day to 50mg/kg/day.
The cross-sensitivity of cephalexin and penicillin is reported to be anywhere from 1% to 10%.1-3 Thus, you may wish to consider other antibiotic options for patients who have a documented history of penicillin allergy. Keflex also is contraindicated in patients with hemophilia and/or other blood disorders due to altered vitamin K absorption.1

|
|
 |
|
| Doxycycline is our first choice for the management of chronic inflammatory conditions, such as rosacea (top) and lid disease (bottom). |
|
3. Doxycycline. If we could prescribe only one oral mediation, it would be doxycycline. This agent is especially useful in treating chronic infections and inflammatory conditions that affect the lids, such as meibomianitis and blepharitis, but also can be used to manage rosacea, chlamydial conjunctivitis and recurrent corneal erosions.
A member of the tetracycline class, doxycycline is bacteriostatic and works by binding to bacterial ribosomes and inhibiting protein synthesis. Clinically, doxycycline is preferred over tetracycline because it is much better absorbed.1,4 Doxycycline should be taken on an empty stomach to further aid absorption.
Doxycycline (and all tetracyclines, in general) are contraindicated in children younger than eight years, nursing mothers and during pregnancy. Clinicians also should keep in mind that pseudotumor cerebri has been documented in patients who use doxycycline––especially in younger individuals.1,5 Increased photosensitivity and gastric distress are other common side effects.
Dosages for doxycycline vary depending upon the patient’s disease state. For severe cases of meibomianitis, consider a dosage of 100mg BID for two to four weeks, followed by 50mg BID for two to four weeks, then 20mg BID for two to four months. Recent studies have indicated that doxycycline dosages as low as 20mg BID are clinically effective, yield fewer side effects and improve compliance.6,7 Thus, we use 50mg BID initially for four weeks, then 20mg BID for three to six months.
For rosacea, 50mg to 100mg daily for two to six weeks should effectively reduce symptoms. Then, the medication can be titrated to 20mg per day as a maintenance dose.
Doxycycline also exhibits anti-inflammatory properties, and reduces the production of inflammatory compounds, such as matrix metalloproteinase (MMP).8 This characteristic makes doxycycline effective against inflammatory lid disease. Studies also have shown that this anti-inflammatory activity can reduce the incidence and severity of recurrent corneal erosions.4,9 A dosage of 50mg doxycycline BID, in conjunction with topical fluorometholone 0.1% TID, for four to eight weeks is recommended to relieve symptoms and decrease recurrence.
Doxycycline is our choice for chronic infectious disease, and can be prescribed as an alternative for acute infections when patients are allergic to penicillin and/or the higher cost of azithromycin is a consideration.
4. Azithromycin. This agent is macrolide antibiotic and derivative of erythromycin. Azithromycin is a first-line treatment for chlamydial infections, such as adult inclusion conjunctivitis and trachoma. For these disease processes, a one-time, a cumulative dose of 1,000mg (four 250mg capsules or two 500mg capsules) should be sufficient.
To treat soft tissue infections, azithromycin can be administered at 500mg for one day and 250mg for four days. Also, it is our first choice for patients with known penicillin or cephalosporin allergies. Azithromycin is safe to use during pregnancy, and is a great alternative to amoxicillin and cephalexin for pediatric patients.
Due to a high rate of azithromycin prescriptions in the US, S. pneumonia and H. influenzae have developed resistance. Several researchers have advocated that prescribing physicians should minimize these prescribing habits.10-12
Furthermore, the FDA has advised clinical discretion, when prescribing azithromycin to patients with a documented history of cardiac problems. Studies have shown that the drug can cause an elongated QT interval, leading to abnormal heart rhythm and possibly death.13
5. Trimethoprim/sulfamethoxazole. A lesser-known but clinically useful oral antibiotic in is trimethoprim/sulfamethoxazole. Given its broad spectrum of activity and effectiveness against S. aureus, this is our drug of choice if MRSA is suspected, for patients with infections that are resistant to other medications and for healthcare personnel. The medication is generally well tolerated, and is dosed just twice a day.
Septra (trimethoprim/sulfa-meth-oxazole, Monarch Pharmaceuticals) and Bactrim (trimethoprim/sulfamethoxazole, Roche) are contraindicated in children less than two months of age, pregnant or nursing mothers, patients with sickle cell disease and those with sulfa allergies. Patients who use either medication may be at a higher risk of Stevens-Johnson syndrome.1
For soft tissue infections in adults, the proper dosage of trimethoprim/sulfamethoxazole is 80mg/400mg to 160mg/800mg BID for 10 to 14 days. Take note that the medication should not be taken with food. Several pediatric options are available for children older than two months; however, the recommended dosage depends on the type and severity of the infection.
|
|
Guidelines for Judicious Oral Analgesics Use
Always be cautious of patients who exhibit drug-seeking behavior. Be wary of those who “self-diagnose” and/or “self-prescribe,” or patients who seek multiple physicians for the same condition. Also, be on the lookout for new patients who present with the exact same illness as someone to whom you recently prescribed narcotics. Other safety measures you might consider include keeping prescription pads safe, not preprinting DEA numbers, not pre-signing Rx pads and writing out numbers (e.g., “ten” vs. “10”). Pay special attention to any pregnant patients who report significant pain. When in doubt, there is no harm in contacting or deferring to the individual’s primary care provider or OB/GYN. Medications that are safe to prescribe in pregnancy include erythromycin, azithromycin, amoxicillin, amoxicillin with clavulanic acid and Tylenol #3, as well as the antiviral medications acyclovir, valacyclovir and famciclovir. |
Oral Analgesics in Eye Care
Conditions such as corneal or conjunctival foreign bodies, corneal abrasions, recurrent corneal erosion, post-refractive surgery, blunt ocular trauma, post-herpetic neuralgia and anterior uveitis could warrant pain management. The options for pain management include over-the-counter medications, prescription medications and heavily regulated narcotic analgesics.
Analgesics either work peripherally (non-steroidal anti-inflammatory drugs and aspirin) at the end receptors or centrally (opioids and acetaminophen) in the nervous system. This fundamental understanding helps us determine the most suitable medication for each patient. We can also take advantage of the different mechanisms of action, as well as the synergistic effect created by using combination medications that include one peripherally- and one centrally-acting agent.
Acetaminophen (Tylenol, McNeil Consumer Healthcare), which is a non-opioid analgesic, helps with pain and fever, but does not exhibit anti-inflammatory properties. The exact mechanism of action is not completely understood, but is thought to work centrally when reducing pain.14
Oral NSAIDs and aspirin, on the other hand, work on the peripheral nervous system by inhibiting cyclooxygenase (COX) at the site of injury.
Opioids act on the central nervous system by blocking incoming nociceptive signals to the brain, thus reducing pain sensitivity. It is worth noting that opioids do not have anti-inflammatory properties.
Our ‘Fabulous Five’ Analgesic Agents
1. Acetaminophen and ibuprofen.
These OTC options are solid choices for basic pain management. The synergistic effect of centrally-acting acetaminophen and peripherally-acting ibuprofen provides excellent pain management. One study indicated that combined ibuprofen and acetaminophen worked more effectively than the concurrent use of an opioid and acetaminophen for pain relief following dental operations.15
The study also showed that the ibuprofen and acetaminophen combination was safer than any analgesic combinations that included opioids.
Over-the-counter Tylenol is the safest pain management option for children and pregnant mothers when used as monotherapy.15 The daily dosage limitation for adults is 4,000mg. Further, Tylenol should not be prescribed to patients who are diagnosed with liver impairment and/or alcoholism.
Ibuprofen dosing should not exceed 2,400mg/day, and should be taken with food if the patient reports gastrointestinal upset.
2. Ketoprofen. At one time, ketoprofen was available OTC. But now, it is a prescription-only NSAID prescribed for mild to moderate pain. It is available in 50mg and 75mg capsules, and typically is dosed every six to eight hours. Additionally, there is a 200mg QD option; however, total daily dosing should not exceed 300mg.
|
|
Contraindications for Narcotic Analgesics
• Known hypersensitivities • COPD • Liver and kidney problems • Pregnancy • History of pain medication abuse |
We have found ketoprofen is especially useful in cases where significant ocular inflammation exists, such as trauma-induced anterior uveitis. Studies have shown that ketoprofen is superior to OTC ibuprofen for pain management, so it is an effective alternative to narcotic analgesics.16
3. Hydrocodone and ibuprofen. Hydrocodone is six times more potent than codeine.17 Unfortunately, with this increased potency comes a profoundly higher likelihood of addiction.
Because of a perceived increase in both drug-seeking behavior and opioid abuse during the last decade, officials from the Drug Enforcement Agency (DEA) reclassified hydrocodone as a Schedule II medication in August 2014. The majority of states only allow optometrists to prescribe Schedule III, IV and V medications.18
It is your responsibility to learn whether you live in a state that still permits ODs to prescribe Schedule II agents. If you are, then Vicoprofen (AbbVie) is our choice. Again, we like taking advantage of the centrally-acting opioid analgesic hydrocodone and the peripherally- acting ibuprofen.
Vicoprofen is available in a 7.5mg/200mg formulation, and can be taken every four to six hours, as needed. Patients should not take more than five tablets per day. Also, Vicoprofen is approved for patients 16 years of age and older.
4. Tylenol with codeine. For those who live in states that do not permit optometrists to prescribe Schedule II medications, we recommend Tylenol with codeine (Janssen Pharmaceuticals). While it does not provide the synergistic analgesic effect associated with hydrocodone and ibuprofen, it does meet our big bottle criteria, and is one of the most frequently prescribed opioid analgesics in the US.
We recommend two formulations––300mg/30mg (Tylenol #3) and 300mg/60mg (Tylenol #4). Tylenol #3 can be prescribed for children older than seven years, and Tylenol 4 can be prescribed for children older than 13 years. If being used long-term, it is prudent to taper the medication to avoid drug dependence.
5. Tramadol. In July 2014, the DEA universally classified tramadol as a Schedule IV medication. Ultram (Janssen Pharmaceuticals) is available in 50mg and 100mg, 200mg and 300mg extended-release dosages. Maximum dosing is 300mg/day for moderate to severe pain.
Oral medications are a wonderful tool for eye care providers. However, each practitioner’s experience, confidence and comfort level with oral prescribing varies dramatically. Involving primary care providers and other medical specialists, as well as pharmacists, can help improve your knowledge of oral medications, appropriate dosing protocols and potential adverse effects.
Our predecessors have worked long and hard to gain oral prescribing rights in clinical practice. Therefore, we encourage you to use them to the fullest scope of your licensure and comfort level to ensure that your patients receive the best care possible.
Dr. Spear owns and operates Sight and Sun Eyeworks, a five-location optometry/ophthalmology practice in Pensacola, Fla.
Dr. Obenchain is in private practice at Sight and Sun Eyeworks in Pensacola.
1. Cooper DH, Krainik AJ, Lubner SJ. The Washington Manual of Medical Therapuetics, 32nd ed. Chapter 12. Antimicrobials. United States: Wolters Kluwer; 2007.
2. Rang HP, Dale MM, Ritter JM, Flower RJ. Rang and Dale’s Pharmacology, 6th ed. Drugs used in the treatment of infection and cancer. China: Elsevier; 2007.
3. Preston SL, Briceland LL. Accuracy of penicillin allergy reporting. Am J Hosp Pharm. 1994 Jan 1;51(1):79-84.
4. Lonsberry B. Doxycycline: Do’s and Don’ts. Rev Optom. 2014 Feb;151(2):38-41.
5. Tabibian JH, Gutierrez MA. Doxycycline-induced pseudotumor cerebri. South Med J. 2009 Mar;102(3):310-1.
6. van Zuuren EJ, Graber MA, Hollis S, et al. Interventions for rosacea. Cochrane Database Syst Rev. 2005 Jul 20;(3):CD003262.
7. Yoo SE, Lee DC, Chang MH. The effect of low-dose doxycycline therapy in chronic meibomian gland dysfunction. Kor J Ophthalmol. 2005 Dec;19(4):258-63.
8. Research in dry eye: report of the Research Subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf. 2007 Apr;5(2):179-93.
9. Wang L, Tsang H, Coroneo M. Treatment of recurrent corneal erosion syndrome using the combination of oral doxycycline and topical corticosteroid. Clin Exp Ophthalmol. 2008 Feb;36(1):8-12.
10. Jenkins SG, Brown SD, Farrell DJ. Trends in antibacterial resistance among Streptococcus pneumoniae
isolated in the USA: update from PROTEKT US years 1-4. Ann Clin Microbiol Antimicrob. 2008 Jan 11;7:1.
11. Hoban DJ, Doern GV, Fluit AC, et al. Worldwide prevalence of antimicrobial resistance in Streptococcus pneumoniae, Haemophilus influenzae
, and Moraxella catarrhalis
in the SENTRY Antimicrobial Surveillance Program, 1997–1999. Clin Infect Dis. 2001;32(Suppl. 2):S81–93
12. Serisier DJ. Risks of population antimicrobial resistance associated with chronic macrolide use for inflammatory airway diseases. Lancet Respir Med. 2013 May;1(3):262-74.
13. U.S. Food and Drug Administration (FDA). Azithromycin (Zithromax or Zmax) and the risk of potentially fatal heart rhythms. FDA Drug Safety Communication, 2013. Available at: www.fda.gov/drugs/drugsafety/ucm341822.htm. Accessed December 28, 2014.
14. Rang HP, Dale MM. Rang and Dale’s Pharmacology, 6th ed. Section 2 – Chemical Mediators: Anti-inflammatory and immunosuppressant drugs. China: Elsevier; 2007.
15. Moore PA, Hersh EV. Combining ibuprofen and acetaminophen for acute pain management after third-molar extractions: translating clinical research to dental practice. J Am Dent Assoc. 2013 Aug;144(8):898-908.
16. Sarzi-Puttini P, Atzeni F, Lanata L, et al. Efficacy of ketoprofen vs. ibuprofen and diclofenac: a systematic review of the literature and meta-analysis. Clin Exp Rheumatol. 2013 Sep-Oct;31(5):731-8.
17. Anderson R, Saiers JH, Abram S, Schlicht C. Accuracy in equianalgesic dosing conversion dilemmas. J Pain Symptom Manage. 2001 May;21(5):397-406.
18. Meers GF, Alldredge BF. Learn to Spot Drug-Seeking Behavior. Rev Optom. Feb;151(2):42-8.
