Every optometrist eventually encounters a patient whose condition causes him or her to lose sleep. If youve been down this road, the questions, Did I diagnose the condition correctly? and Is my treatment working? may have haunted you until the patients follow-up appointment.
Below, Dr. Kabat discusses three challenging and severe cases: a patient with an extreme case of bacterial keratitis that invaded the visual axis; a seemingly binocular vision case that turned out to be a life-threatening condition; and a patient with a corneal abrasion that worsened due to inappropriate initial treatment.
Case: I Swear I Didnt Sleep in My Contacts
A 15-year-old Hispanic female presented with unilateral redness. She reported pain and decreased vision in her right eye.
Examination
On examination, this patients visual acuity measured 20/400 in the right eye and 20/20 in the left eye. Her fields were full to confrontation, and her motilities were full and equal. Her ocular and medical histories were unremarkable. She reported wearing contact lenses for the past three months and claimed to comply with an appropriate contact lens care regimen. She also said that she did not sleep in her lenses. The examination, however, suggested otherwise.
 |
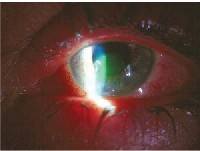
| Patients right eye has a dense infiltrative keratitis with overlying epithelial defect. |
Dr. Kabat diagnosed a dense infiltrative keratitis with overlying epithelial defect on the patients right eye. We must assume that corneal ulcers that present in this fashion are bacterial (i.e., bacterial keratitis) until proven otherwise, Dr. Kabat says.
Given that this patient wears contact lenses and lives in southern Florida, Dr. Kabat suspected that Pseudomonas aeruginosa, a gram-negative bacteria, was the offender. P. aeruginosa is less common than Staphylococcus aureus and Streptococcus pneumoniae, but it is often associated with contact lens wear and is common in warm, moist climates. P. aeruginosa is more aggressive than most gram-positive bacteria, and it tends to invade the visual axis. In cases such as this, obtaining cultures is indicated.
In addition to severely decreased acuity, this patients eye was so in-flamed from the bacterial infection that she also developed an anterior chamber reaction (i.e., secondary uveitis), causing a hypopyon to develop. Bacterial keratitis is not uncommon, particularly in patients who wear contact lenses, Dr. Kabat says. However, severe central ulcers pose two significant risks. The first risk is permanent corneal scarring. An ulcer of this magnitude is likely to leave a scar, which leads to visual impairment if the visual axis is involved. The second risk is corneal thinning and perforation, which can lead to loss of the eye. Because this is risky business, Dr. Kabat says the attending O.D. has two options: treat the condition immediately and aggressively, or refer the patient to someone who can.
Signs and Symptoms
According to Dr. Kabat, signs and symptoms of bacterial keratitis include:
Conjunctival and episcleral injection.
Focal corneal infiltrate with overlying epithelial defect.
Severe anterior chamber reaction.
Mild mucopurulent discharge.
Corneal edema.
Reduced visual acuity.
Extended contact lens wear.
Corneal trauma or insult.
Pain.
Photophobia.
Lacrimation.
Blurred vision.
Pathophysiology
Bacterial keratitis begins when a bacterial pathogen gains entry to the cornea. This process is known as stromal induction. Contact lenses can cause microabrasions in the epithelium that enable bacteria to enter the cornea. As bacteria proliferate, inflammation and corneal damage can occur. This happens because white blood cells infiltrate the corneal stroma in an attempt to fight off invading bacteria, says Dr. Kabat. But, these white blood cells also damage the cornea by their presence, and the inflammatory effect induces collagenolysis, which causes the cornea to begin breaking down. Therefore, to properly manage a corneal ulcer, the bacteria must be neutralized and the inflammatory response must be quelled.
Management
Bacterial keratitis should be treated with both a broad-spectrum antibiotic and a potent corticosteroid, Dr. Kabat says. The antibiotic serves to destroy the bacteria, while the corticosteroid addresses the inflammatory response. The following antibiotics are FDA approved to treat bacterial keratitis:
Fortified aminoglycosides and cephalosporins. These drugs were the standard treatments for bacterial keratitis before fluoroquinolones were introduced.
Ciloxan (ciprofloxacin 0.3%, Alcon).
Ocuflox (ofloxacin 0.3%, Allergan).
Iquix (levofloxacin 1.5%, Santen). This drug has been FDA approved for the treatment of bacterial keratitis, but it is not yet available on the market.
Many practitioners now also use the two fourth-generation fluoroquinolones off-label to treat bacterial keratitis. These are:
Vigamox (moxifloxacin 0.5%, Alcon).
Zymar (gatifloxacin 0.3%, Allergan).
Vigamox and Zymar may be used in the same way as older-generation drugs, says Dr. Kabat. First, provide the patient with a loading dose (i.e., several drops while he or she is in your office). Then, dose one drop every 15 minutes to one hour, depending on the severity of the corneal ulcer, for the remainder of the day. Continue dosing every one to four hours overnight. You can modify the regimen depending on the resolution of the ulcer, but never administer the drug less than q.i.d. because sublethal dosing promotes the development of bacterial resistance.
Because the organisms are embedded in the cornea, bacterial keratitis requires more frequent instillation of an antibiotic than does conjunctivitis. If the corneal ulcer is stabilized or resolving 24 hours after initiating antibiotic treatment, only then does Dr. Kabat recommend adding a corticosteroid to reduce inflammation.
Dr. Kabat administered a loading dose of Vigamox (i.e., two drops) to this patient and told her to administer one drop every hour while awake and one drop every three hours overnight. He saw her the next day and told her to continue using Vigamox hourly. He also added Pred Forte (predniso-lone acetate 1.0%, Allergan) one drop every hour while awake, alternating on the half-hour with Vigamox.
Dr. Kabat saw this patient daily for the next five days to ensure that her condition was improving. On day six, there was significant resolution, and
both drugs were reduced to q.i.d. dosing. After four more days of this treatment, the inflammation was eradicated and the epithelium was healed, so the medications were discontinued.
Outcome
This patients corneal ulcer resolved within 10 days of her initial visit with this therapy, says Dr. Kabat. At this point, he referred her to the contact lens department for re-evaluation of her lens fit and to re-emphasize the importance of an appropriate contact lens wear schedule. Two weeks after her first visit, her visual acuity was 20/30 O.S., which is remarkable considering her initial presentation, says Dr. Kabat. Remember that patients with central ulcers should expect to have some degree of diminished acuity, even with proper treatment. Dr. Kabat always advises patients of this, and then works aggressively to restore vision to its fullest.
When managing patients who have severe bacterial keratitis, Dr. Kabat recommends that you remember the following:
Small corneal lesions with disproportionate inflammation, patient discomfort and overlying staining are corneal ulcers and should be treated as such.
Always manage bacterial keratitis promptly and aggressively.
Empirical antibiotic therapy is acceptable in most cases, but obtain a culture in certain situations (see When to Culture).
Always employ corticosteroids after sufficient antibiosis has been achieved, usually on day two or three. Corticosteroids will not cause the infection to worsen, but they will quell the inflammatory response, which can threaten vision.
| When to Culture Obtain cultures if: Central ulcers are severe. Ulcers show impending perforation. Corneal ulcers are not responding to therapy. The bacterial strain could be resistant. You are not comfortable with empiric treatment. Patients are in institutional settings. Resistant bacterial strains are more likely to be present in institutional settings, and may not respond to conventional drugs. AK |
Case: Not Another Binocular Vision Case!
A 17-year-old black female presented and reported that she was experiencing intermittent double vision, primarily while reading. She reported having this problem for the past three months and said it seemed to be worsening. She also reported experiencing occasional headaches, which she thought were associated with reading. She denied any eye pain and neurological symptoms, including nausea, vomiting, motor weakness and paraesthesias. Her ocular and medical histories were unremarkable.
Examination
This patients visual acuity measured 20/20 O.U. Biomicroscopy, tonometry and ophthalmoscopy results were normal. Her motility was full in the right eye, but her left eye showed mild underaction in left lateral gaze (i.e., an abduction deficit). Dr. Kabat performed a forced-duction test in which he tried to move her left eye. The result was negative (i.e., he could move it, but she could not), which implied muscle weakness or a nerve problem.
Diagnosis
This patient demonstrated a left abduction deficit, suggesting that either her sixth nerve or medial rectus muscle were not working properly. The forced duction test all but confirmed a sixth nerve (abducens) palsy, Dr. Kabat says.
Signs and Symptoms
According to Dr. Kabat, classic signs and symptoms of sixth nerve palsy with an intracranial pathology may include:
Papilledema.
Nausea.
Vomiting.
Tinnitus.
Pronounced headaches.
Pathophysiology
Sixth nerve palsy has several possible etiologies. In adults, the most common cause of acute-onset, non-traumatic sixth nerve palsy is ischemic-vascular disease, such as diabetes. In children and young adults, the most common cause is a mass lesion of the central nervous system, followed by multiple sclerosis, viral infection and pseudomotor cerebri. Significant intracranial pathology may be present even when classic signs and symptoms are absent, says Dr. Kabat.
Management
Young patients (i.e., those younger than age 30) with acute-onset sixth nerve palsy warrant immediate neuro-imaging because a mass lesion is likely implicated, Dr. Kabat says. He immediately sent this patient for an MRI. Then, he consulted with her neurologist.
MRI revealed a golf ball-sized mass growing within her cerebral ventricular system in the fourth ventricle. The mass prevented outflow of cerebral spinal fluid, so pressure was building. This abnormal accumulation of fluid is known as hydrocephalus.
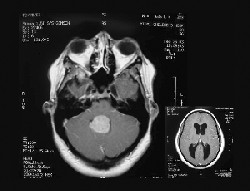 |
| MRI revealed a mass growing within this patients cerebral ventricular system. |
A neurosurgeon removed the mass, which was found to be a choroid plexus papillomaa benign tumor. Although the mass did not invade other parts of her brain, the hydrocephalus could have caused death. After her surgery, the diplopia abated. The patient recovered fully and remains in good health.
Clinical Pearls
Something as seemingly benign as double vision in a child can be a significant problem and warrants further investigation.
Sixth nerve palsy is a frequent cause of neurogenic diplopia.
Young patients with acute-onset sixth nerve palsy warrant immediate neuro-imaging. If youre unsure about a diagnosis, refer the patient for neuro-imaging. Not all patients will have classic symptoms, such as nausea, vomiting and headaches.
Case: Agave Myself an Abrasion
A 44-year-old white female presented with a very painful, red left eye, four hours after she poked it with a pointy agave plant.
Examination
This patients visual acuity measured 20/30 in her left eye, and her motilities were full. She had limbal injection and a mild anterior chamber reaction. During her slit lamp examination, Dr. Kabat saw a 5mm vertical abrasion with ragged edges on the central cornea of her left eye.
 |
| This patients left eye had a 5mm vertical abrasion with ragged edges on the central cornea. |
Dr. Kabat treated this patient with cyclopentolate, as it was the only cycloplegic available to him at the time. However, it was not the appropriate treatment for her corneal abrasion. He also administered two drops of Ocuflox to prevent infection, and two drops of the NSAID Voltaren (diclofenac sod-ium 0.1%, CIBA Vision) to alleviate the patients pain. He then bandaged her left eye with a soft contact lens and instructed her to continue using Ocuflox and Voltaren every four hours. A follow-up visit was scheduled for the next morning.
Later that evening, the patient paged Dr. Kabat because she was still experiencing excessive pain. When she arrived at his clinic, she had severe corneal edema and a flapping epithelium. Since the abrasion occurred only a few hours before her initial appointment, Dr. Kabat had hoped that the soft contact lens would tack down the loose epithelium. However, he soon learned that this does not happen in corneal abrasions. The minute the epithelium loses contact with the underlying stroma, it begins to die, becoming antigenic and initiating an inflammatory response. Seeing how the situation had deteriorated, Dr. Kabat elected to debride the abrasion. He then administered Pred Forte and 0.25% scopolamine in-office to reduce the inflammation. He reapplied a bandage contact lens and prescribed 800mg of ibuprofen (the maximum recommended dosage) to ease her pain. The following morning, she looked and felt better, says Dr. Kabat.
To effectively manage corneal abrasions, Dr. Kabat recommends:
Quelling the inflammatory cascade with a potent cycloplegic agent, such as 0.25% scopolamine.
Facilitating re-epithelialization by removing loose, dead epithelium.
Preventing secondary infection with an antibiotic.
Clinical Pearls
Always remove loose epithelium associated with corneal abrasions. Loose epithelium is non-viable tissue, and it will become antigenic if left behind.
Antibiotics are prophylactic and not therapeutic in situations like this, so administer them accordingly. Remember too that antibiotics, particularly those preserved with benzalkonium chloride, can be corneotoxic and delay re-epithelialization if used excessively.
Steroids and NSAIDs are important to manage pain and secondary inflammation.
To modify a line from the film Forrest Gump, Optometry is like a box of chocolates. You never know what youre going to get. In other words, you never know what will walk into your office on any day, and if what you are seeing and hearing from a patient represents the entire story. So, always be prepared to encounter extreme and challenging cases, and know how to respond to ensure the safety and well-being of your patients.
