 |
Q:
I have a 64-year-old female patient with irregular astigmatism due to map-dot-fingerprint dystrophy who needs cataract surgery. Is she a candidate for a toric lens?
A:
Advising a cataract patient on the best intraocular lens (IOL) options depends on several factors, many of which are revealed with corneal topography, according to Steven Sorkin, OD, of Corneal Associates of New Jersey. “Corneal topography is a must-do test prior to referring patients for cataract surgery” to detect patients who may be eligible for a toric lens vs. those with irregular cylinder and various corneal conditions that would rule these options out, Dr. Sorkin says.
Toric IOLs
These lenses play a huge role in cataract correction, and higher cylinder corrections are readily available to treat one to four diopters of regular corneal astigmatism, says Dr. Sorkin. Regular astigmatism can also now be corrected, up to about two diopters, in patients who want to explore a multifocal or presbyopic lens option.
However, multifocal lenses (with or without astigmatism correction) are not good options for patients whose corneal cylinder is irregular from ocular surface disease, dystrophies or degenerations.
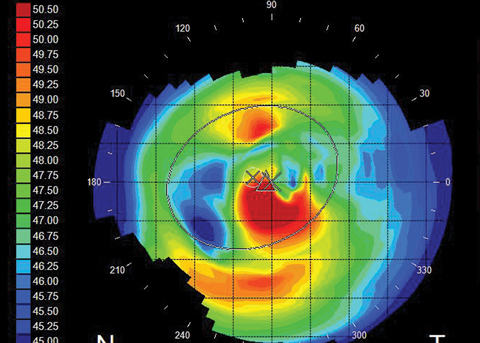 |
| Fig. 1. Irregular astigmatism caused by map-dot-fingerprint dystrophy. Click image to enlarge. |
Distortion’s Causes
Anything from contact lens overwear to Salzmann’s nodular degeneration and even map-dot-fingerprint dystrophy can cause corneal distortion and irregular astigmatism—a major concern that must be addressed before cataract surgery, Dr. Sorkin explains. “Just as important, ocular surface disease can induce topographical changes, as the measurements are affected by dry spots on the cornea.” Also, superficial punctate keratitis, ptyergia and lid abnormalities such as chalazia can manifest as distortion on corneal topography, he adds.
He explains that contact lenses such as thick toric soft lenses and long-term gas permeable lens wear can cause corneal warpage due to hypoxic stress. “Corneal warpage will show up on topography as irregular astigmatism and distortion,” says Dr. Sorkin. Contact lens wear must be discontinued for a period of time to allow the cornea to stabilize prior to cataract surgery. “Soft lenses should be discontinued a minimum of two weeks. Gas permeable contact lenses may need to be discontinued for a month or more until keratometry and topography is stabilized over multiple visits,” says Dr. Sorkin.
Optimize the Surface
Before referring the patient, it is imperative to “clean up” the lids and corneal surface, as accurate measurements must be obtained to prevent refractive surprises and suboptimal post-op acuity, Dr. Sorkin explains. Aggressive ocular surface treatment with an appropriate combination of options that may include lubrication, Restasis (cyclosporin A, Allergan) or Xiidra (lifitegrast 5%, Shire), punctal plugs, eyelid hygiene, essential fatty acid supplementation, hypochlorous lid scrubs and Lipiflow (Tearscience) “can help optimize the ocular surface prior to surgery,” says Dr. Sorkin.
This Patient’s Options
The 64-year-old patient in question expressed a desire to get a toric IOL for clear unaided distance vision. However, she would not be a good candidate for this lens due to her map-dot-fingerprint dystrophy. This is something best explained in advance by you, her primary care eye optometrist, according to Dr. Sorkin. The highly irregular topography would prevent accurate readings, and the outcome would be less than optimal (Figure 1).
If the optometrist didn’t perform corneal topography, it would be impossible to counsel the patient on the best lens choice for their particular situation. The patient might get their hopes up for a premium lens only to be turned down by the surgeon, a frustrating and embarrassing moment for all.
