 |
History
A 27-year-old Caucasian male reported to the office with a chief complaint of “pink eye.” He explained that his eyes became red following a cold two weeks earlier and that Visine (tetrahydrozoline, Johnson & Johnson) made them less red but didn’t stop the discharge.
His systemic and ocular histories were unremarkable and he denied exposure to chemicals or allergens of any kind.
Diagnostic Data
His best-corrected entering visual acuities were 20/20 OU at distance and near. His external examination was normal with no evidence of afferent pupillary defect.
The biomicroscopic examination of the anterior segment is demonstrated in the photographs. Goldmann applanation tonometry measured 15mm Hg OU.
The dilated fundus findings were normal peripherally and centrally with normal nerves and maculae.
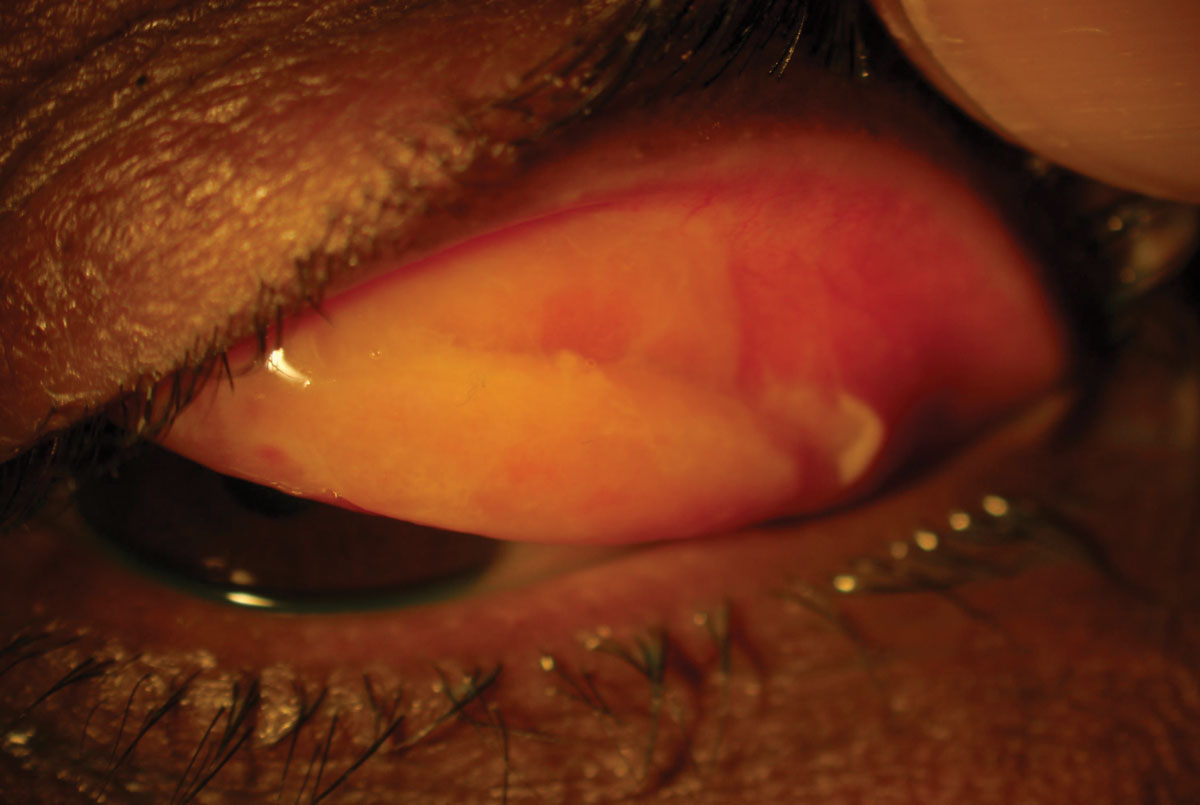 |
| This 27-year-old patient’s persistent reddening and discharge was coupled with this finding, seen upon everting the eyelid. Click image to enlarge. |
Discussion
Additional studies included corneal sensitivity testing, to rule out chronic conjunctival disease, and eyelid eversion, to rule out superior palpebral conjunctival involvement or scarring. Sodium fluorescein staining was completed to assess the status of the corneal epithelium. Culturing was plausible to uncover the presence of adenoviral antigens but was not done in this case. Finally, the preauricular lymph nodes were evaluated for tenderness and swelling.
The diagnosis in this issue is conjunctivitis with pseudo-membrane. Conjunctivitis can be generically described as swelling of the bulbar, fornix or palpebral conjuctival tissues. Isolated infection (bacterial or viral), toxic exposure to ultraviolet light, toxic exposure to solid, liquid or gaseous substances, auto inflammatory disease, ischemic processes or combinations of these etiologies have all been implicated as causative.1-6 The tissue’s clinical appearance along with the symptoms will be variable dependant upon the cause but generically may include itchy, irritated, scratchy discomfort in the setting of watery, stringy or mucopurulent discharge, hyperemia, follicles and papillae along with a mild inferiorly-based keratitis with or without subepithelial inflitraton.1-14
Pseudomembrane or membrane formation in association with conjunctivitis can occur anytime there is significant damage to the conjunctival surface (toxic/chemical exposure, Stevens-Johnson syndrome, ocular pemphigoid, frictional exposure to foreign matter); however, it classically associated with four principle etiopathologies: adenovirus conjunctivitis or epidemic keratoconjunctivitis, bacterial or acute infectious conjunctivitis, ligneous conjunctivitis and graft-vs.-host disease (GVHD).1-15 The pseudo or true membrane that forms does not typically alter the symptoms experienced by the patient unless it is discharged from the palpebral fissure impacts the ability of the eyelids to perform their function. If the conjunctival fornicies are forshortened and symblepheron develops, ocular surface sequellae which include ocular dryness, discomfort and variable visual disturbances will follow. If the pseudomembrane or membrane disturbs the integrity of the cornea, mechanical ulceration by proximity is plausible.2
Distinguishing Etiopathologies
Epidemic keratoconjunctivitis (EKC) may present as a unilateral or bilateral, inferior palpebral, follicular conjunctivitis with epithelial and subepithelial keratitis and normal corneal sensation.11,12 When subepithelial infiltrates (SEI) are seen, they are typically concentrated in the central cornea, uniquely sparring the periphery.11,12 Conjunctival injection, tearing, watery discharge, red edematous eyelids, pinpoint subconjunctival hemorrhages, pseudomembrane (with occasional true membrane) formation and palpable preauricular, submandibular, or submental lymph nodes are fundamental clinical signs of the entity.10-12 In severe cases, conjunctival desiccation can result in scarring of the palpebral and fornix conjunctiva.11 The condition is known for its contagiousness.10-12
Gonococcal conjunctivitis (gonococcal keratoconjunctivitis when the cornea is also involved), is sometimes referred to as hyperacute conjunctivitis.9 While most cases are the result of sexually transmitted vectors, infected individuals have been detected without evidence of genital signs or symptoms.16 The medical literature has recorded communal baths, towels or fabrics, rectal thermometers and poorly sanitized caregivers hands as an alternate means of transmission.17 The contagious ocular disease typically presents as an acute, red eye with severe muco-purulent discharge of less than 4 weeks duration.9 Conjunctival papillae, superficial punctate keratitis and marked chemosis are almost always present.9,10,16-19 Subconjunctival hemorrhage (hemorrhagic conjunctivitis), pseudo or true membrane formation and preauricular adenopathy are usually present.9,10,16-20 In chronic, recalcitrant or severe cases, peripheral subepithelial corneal infiltration may occur leading to corneal ulceration with anterior iritis.10
Ligneous conjunctivitis is a rare form of chronic conjunctivitis characterized by the development of firm fibrin-rich, wood-like pseudomembraneous lesions on the tarsal conjunctiva of one or both eyes.3 Less frequently, similar lesions may occur on other mucous membranes of the body indicating that these manifestations are part of a systemic disease.3 Plasminogen deficiency (hypoplasminoginaemia), congenital occlusive hydrocephalus and juvenile colloid milium are other systemically associated disorders.3 An autosomal recessive inheritance pattern is reported in the literature.20,21 Here, the developing intrusive matter organizes and attaches to the underlying tissues mechanically inducing trauma to the ocular surfaces where it has exposure. Foreign body sensation, keratopathy and corneal ulceration are all plausible.3,5 Ligneous conjunctivitis has been induced by oral antifibrinolytic treatment with tranexamic acid.3
Hematopoietic stem cell transplantation (HSCT) is a treatment for multiple medical conditions that result in bone marrow failure.22 GVHD is a complication of allogeneic (taken from different individuals of the same species) hematopoietic stem cell transplantation. GVHD can be considered an exaggerated, undesirable manifestation of the normal inflammatory mechanism where donor lymphocytes encounter foreign antigens in a milieu that fosters inflammation.23,24 The fundamental interaction of the GVHD response is the interaction of donor T cells with host antigen presenting cells (APC).25 Cytokines, chemokines and immune cell subsets also play a role.24 In the eye the lacrimal gland and conjunctival surfaces can be affected inducing dry eye, conjunctival scarring and in severe cases, pseudomembrane induction.14,15,21-23
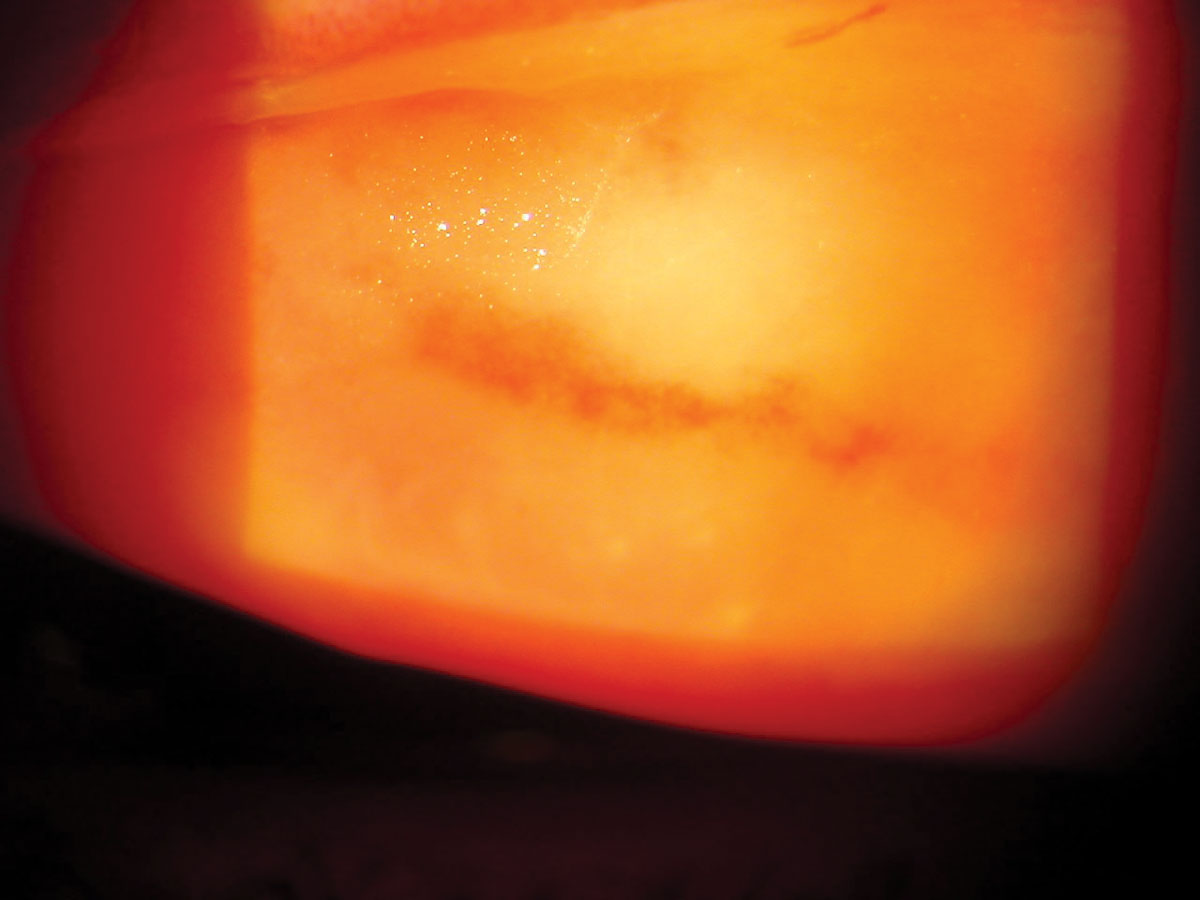 |
| Did you identify the underlying condition causing this patient's distress? Click image to enlarge. |
Dealing With Pseudomembranes
While the etiopathology of the conjunctivitis might vary, the base histochemical error that permits conjunctival pseudomembranes and membranes to form is the same.3-6,15 Pseudomembranes and “true” membranes are composed of the same materials (fibrinogen, granulation tissue, and inflammatory cells) and are only differentiated by the amount of organized exudate that is coagulated and its interdigitation with the underlying tissue.15,25 A “true” membrane is composed of a greater amount of fibrin. By way of the inflammatory response and time, the constituents comingle with both the necrotic epithelium and the substantia propria of the affected tissue. This makes “true” membranes more difficult to remove, increasing both the likelihood and volume of bleeding upon their extraction.15 This is a documented clinical diagnostic feature.15
Affected humans who become plasminogen-deficient through congenital disease or an acquired process undergo aberrant wound healing, mainly within injured mucosal tissue.3 Here, impaired plasmin-mediated extracellular fibrinolysis (the disassembly and demolition of unneeded fibrin) results in the deposition of “wood-like” plaque material onto the affected tissues. Pseudomembraneous lesions of the eyes and other mucosal tissues mainly contain clotted fibrin(ogen).3
Plasminogen deficiency has emerged as a well-recognized disorder in which reduced levels of plasminogen lead to the development of pseudo membranes on mucosal surfaces.4 Two types of plasminogen deficiency have been described in the literature. Type I represents a quantitative deficiency and type II a qualitative deficiency.4
In cases of pseudomembrane or membrane formation secondary to forms of conjunctivitis where there is no plasminiogen deficiency, the exudates and inflammatory response produced by the conjunctivitis itself creates volumes of the substances that form the scaffolding of the process.5 Pseudomembranes or membranes are comprised of fibrin, chemical mediators of inflammation such as matrix metalloprotinases (MMP) and other inflammatory cells, however, both direct and indirect evidence implicates some mechanism of hypofibrinolysis as the primary defect.5
The appropriate method of resolving conjunctivitis with pseudomembrane or “true”membrane has two components: 1). Appropriately diagnose and treat the underlying cause of the conjunctivitis and 2). Remove the pseudo or “true” membranes from the conjunctival surfaces.
Management
Viral conjunctivitis is contagious but self-limiting. The primary function of management is to increase patient awareness and comfort by providing education and decreasing symptomatology.26 Patients should be kept home from work or school until contagious discharge is eliminated.26 Patients should be warned not to use common utensils, glasses, linens or wash cloths. Medical management may range from supportive cold compress and tears, as needed to topical vasoconstrictors, topical nonsteroidal anti-inflammatory medications and steroids BID to QID. If pseudo or true membranes are present they should be peeled using a moistened cotton tipped applicator soaked in a combination of antibiotic and anesthetic solution. Forceps can be used as well for pseudo or “true” membranes that will not separate from the conjunctival tissue with a contton-tipped applicator alone. Topical antibiotic/steroidal combination therapy QID or separate drops in the same respective classes can be employed following the removal of the false tissue.11
In cases of hyperacute or sexually transmitted conjunctivitis options include oral tetracycline 250mgs to 500mgs, QID, PO for three weeks or its alternatives (doxycycline, minocycline, azothromicin) along with a topical antibiotic (fourth generation fluorinated quinolone), qid-q2h, topical steroidal preparations qid-q2h and cycloplegic preparations, QD to TID, as necessary. Since tetracycline requires considerations such as administration one hour before or after meals to avoid gastrointestinal side effects, interference of dairy products with its effectiveness and ability to deform bones and teeth in the young (less than 10 years old), its alternatives may present a better option. Amoxacillin and erythromycin, 250mgs to 500mgs, QID, PO for three weeks or doxycycline, 100mgs, BID, for one week are acceptable alternatives.17,27-30 Ceftriaxone, cefixime, spectinomycin and azithromycin (one gram) are all acceptable alternatives which may be required should suspicion of resistant strains of gonorrhea or chlamydia be suspected.31,32 Medical management of gonococcal conjunctivitis begins with an intramuscular loading dose of ceftriaxone, one gram.31-33 Ideally, therapy should continue with hospital admission and intravenous administration of Ceftriaxone 1 gram Q 12 to 24 hours.34 The oral antibiotics are added subsequently following discharge.31-33
Mechanical removal of all discharge and debris is a critical element to both the success of infection resolution and improving patient functioning. The eyelids should be everted to rule out the presence of pseudomembranes. Remove pseudomembranes if discovered via the method described previously. Over-the-counter oral analgesics can be used to increase patient comfort along with palliative measures such as cold compresses and ocular lubricants.
For ligneous conjunctivitis, a plasminogen concentrate formulated into an ophthalmologic preparation has been found to be an effective local therapy. Unfortunately, no plasminogen concentrate is currently available commercially for either systemic or local therapy.4
GVHD produces ocular sequellae consistent with tear dysfunction syndrome.34 Artificial tear solutions, ointments, puntal plugs, oral medications increase tear and goblet cell function are all reasonable. A report in the literature suggests that 0.05% topical cyclosporin may be an effective treatment for for these individuals.34 Pseudo or “true” membranes should be removed via the method described previously.
1. Uchio E. New medical treatment for viral conjunctivitis. Nippon Ganka Gakkai Zasshi. 2005;109(12):962-84. 2. Uchino M, Ogawa Y, Kawai M, et al. Ocular complications in a child with acute graft-versus-host disease following cord blood stem cell transplantation: therapeutic challenges. Acta Ophthalmol Scand. 2006;84(4):545-8. 3.Schuster V, Seregard S. Ligneous conjunctivitis. Surv Ophthalmol. 2003;48(4):369-88. 4. Mehta R, Shapiro AD. Plasminogen deficiency. Haemophilia. 2008;14(6):1261-8. 5. Ramsby ML, Donshik PC, Makowski GS. Ligneous conjunctivitis: biochemical evidence for hypofibrinolysis. Inflammation. 2000;24(1):45-71. 6. Lijnen HR. Elements of the fibrinolytic system. Ann N Y Acad Sci. 2001;936(6):226-36. 7. Tarabishy AB, Jeng BH. Bacterial conjunctivitis: a review for internists. Cleve Clin J Med. 2008;75(7):507-12. 8. Sheikh A, Hurwitz B. Antibiotics versus placebo for acute bacterial conjunctivitis. Cochrane Database Syst Rev. 2006;19(2):CD001211. 9. Ullman S, Roussel TJ, Forster RK. Gonococcal keratoconjunctivitis. Surv Ophthalmol. 1987;32(3):199-208. 10. Thatcher RW. Treatment of acute gonococcal conjunctivitis. Ann Ophthalmol. 1978;10(4):445-9. 11. Uchio E, Takeuchi S, Itoh N, et al. Clinical and epidemiological features of acute follicular conjunctivitis with special reference to that caused by herpes simplex virus 12. Murrah WF. Epidemic keratoconjunctivitis. Ann Ophthalmol. 1988;20(1):36-8. 13 Karki DB, Shrestha CD, Shrestha S. Acute haemorrhagic conjunctivitis: an epidemic in August/September 2003. Kathmandu Univ Med J (KUMJ). 2003;1(4):234-6. 14. Rashid S, Dana MR. Cicatrizing and autoimmune diseases. Chem Immunol Allergy. 2007;92:195-202. 15. Volcker HE, Naumann GOH. The conjuctiva. In: Naumann GOH. Pathology of the eye. Verlag, Germany, Springer 1986: 249-316. 16. Annan NT, Boag FC. Outpatient management of severe gonococcal ophthalmia without genital infection. Int J STD AIDS. 2008;19(8):573-4. 17. Goodyear-Smith F. What is the evidence for non-sexual transmission of gonorrhoea in children after the neonatal period? A systematic review. J Forensic Leg Med. 2007;14(8):489-502. 18. Woods CR. Gonococcal infections in neonates and young children. Semin Pediatr Infect Dis. 2005;16(4):258-70. 19. Kohl PK. Gonorrhea. Urologe A. 2006;45(12):1501-3. 20. Francois J. Considerations on the importance of genetics in ophthalmology. Ophthalmologica. 1979;178(6):381-95. 21. Schuster V, Hügle B, Tefs K. Plasminogen deficiency. J Thromb Haemost. 2007;5(12):2315-22. 22. Ogawa Y, Dogru M, Uchino M, et al. Topical tranilast for treatment of the early stage of mild dry eye associated with chronic GVHD. Bone Marrow Transplant. 2010;45(3):565-9. 23. Ferrara JL, Reddy P. Pathophysiology of graft-versus-host disease. Semin Hematol. 2006;43(1):3-10. 24. Choi S, Reddy P. Graft-versus-host disease. Panminerva Med. 2010;52(2):111-24. 25. Yohe SL, Reyes M, Johnson DA, et al. Plasminogen deficiency as a rare cause of conjunctivitis and lymphadenopathy. Am J Surg Pathol. 2009;33(2):313-9. 26. Aoki K, Tagawa Y. A twenty-one year surveillance of adenoviral conjunctivitis in Sapporo, Japan. Int Ophthalmol Clin. 2002;42(1):49-54. 27. Darville T. Chlamydia trachomatis infections in neonates and young children. Semin Pediatr Infect Dis. 2005;16(4):235-44. 28. Meyers DS, Halvorson H, Luckhaupt S, et al. Screening for chlamydial infection: an evidence update for the U.S. Preventive Services Task Force. Ann Intern Med. 2007;147(2):135-42. 29. Zar HJ. Neonatal chlamydial infections: prevention and treatment. Paediatr Drugs. 2005;7(2):103-10. 30. Quirke M, Cullinane A.Recent trends in chlamydial and gonococcal conjunctivitis among neonates and adults in an Irish hospital. Int J Infect Dis. 2008;12(4):371-3. 31. Chen PL, Hsieh YH, Lee HC, et al. Suboptimal therapy and clinical management of gonorrhoea in an area with high-level antimicrobial resistance. Int J STD AIDS. 2009;20(4):225-8. 32. Agence française de sécurité sanitaire des produits de santé (Afssaps). Antibiotherapy applied to uncomplicated urethritis and cervicitis. French Agency for Health Product Safety. Med Mal Infect. 2006;36(1):27-35. 33. Skolnik, N.S. Screening for Chlamydia Trachomatis Infection. American Family Physician 1995;52(1):95. 34. Wang Y, Ogawa Y, Dogru M, et al. Ocular surface and tear functions after topical cyclosporine treatment in dry eye patients with chronic graft-versus-host disease. Bone Marrow Transplant. 2008;41(3):293-302. |
