|
Q:
A glaucoma patient called the office stating that she rubbed her eye and a “piece of plastic came out.” What is going on?
“Advanced glaucoma patients can be a challenge from a treatment standpoint,” says Justin Schweitzer, OD, of Vance Thompson Vision in Sioux Falls, SD. “Like this case, these patients have had glaucoma for a long time. They have maxed out on medications, had multiple selective laser trabeculoplasties, stents, goniotomies and, still, they continue to progress.”
Enter our more advanced glaucoma surgeries, tube shunts and trabeculectomies. These procedures are great from an efficacy standpoint but carry a higher complication profile than other glaucoma treatment options. The Tube vs. Trabeculectomy Study Group revealed that 39% of patients in the tube group and 60% of patients in the trabeculectomy group had postoperative complications.1 These include diplopia, iritis, hypotony, infection, bleb leaks and exposures. In this study, tube erosion occurred in 5% of patients in the tube shunt group.1 In another study, exposure of the tube and/or plate is estimated to occur in approximately 2.5% to 8.9% of cases.2 Exposure is one of the most serious complications due to the risk of vision-threatening endophthalmitis.
 |
|
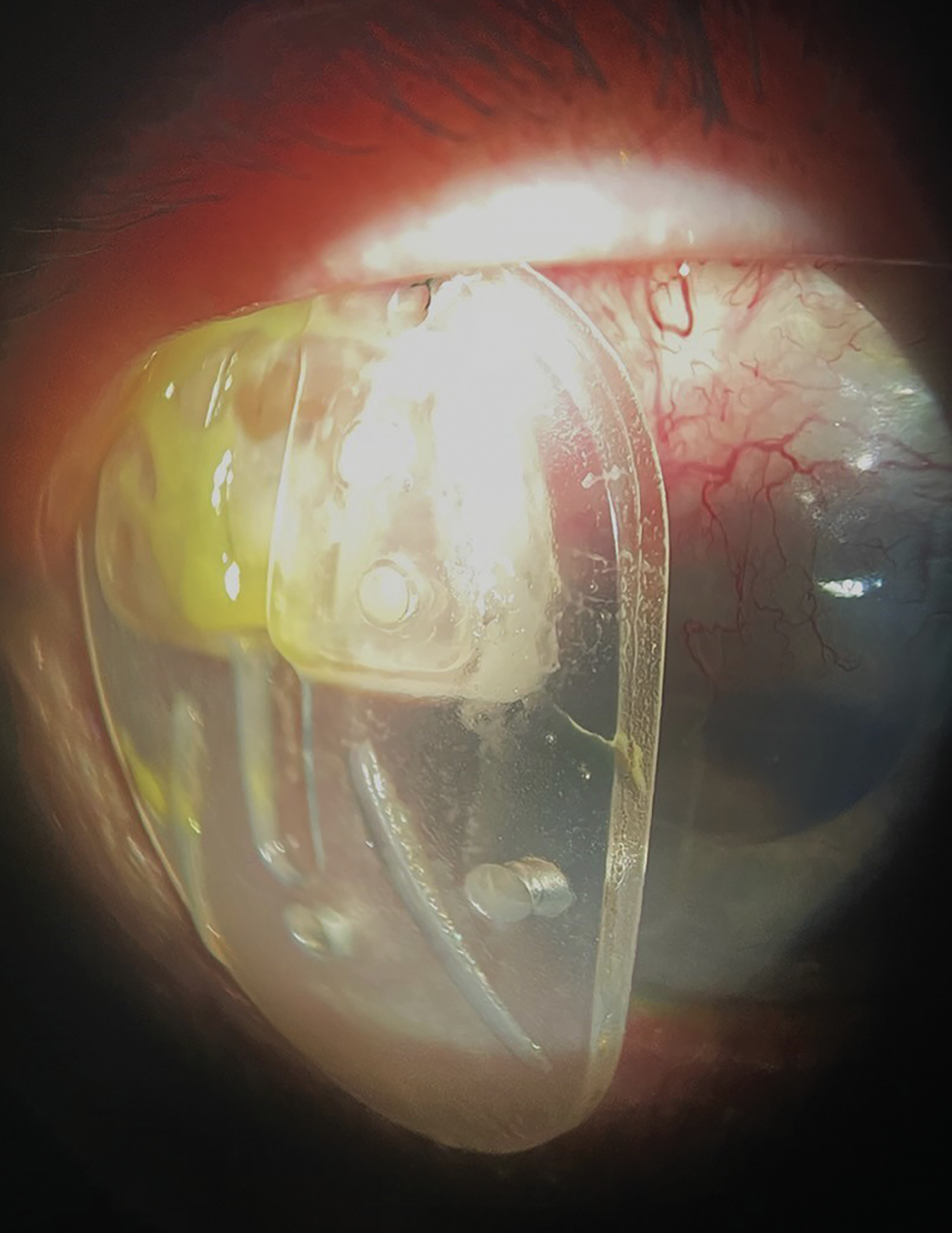
Ahmed valve after it was expulsed from the eye seven weeks post-op. Click image to enlarge. |
“Our patient was seven weeks post-surgery, meaning that a combination of etiologies could be in play that led to the total expulsion of the shunt,” Dr. Schweitzer notes. “Eye rubbing, micro-movements due to blinking or ocular movements, or incomplete healing can lead to an erosion of the overlying conjunctiva or the patch graft over the plate.”
Management
The level of exposure will dictate whether immediate repair needs to occur or if medical management can be attempted. Erosions can be small (millimeter), large (3mm to 5mm) or, like this patient, a complete exposure. She had a true emergent complication that needed immediate repair. In the clinic, initiate a topical antibiotic every one hour to reduce the risk of endophthalmitis. Dr. Schweitzer recommends closing the eyelid with a taped tarsorrhaphy will hopefully prevent further movement of the tube shunt until the patient can see the glaucoma surgeon.
Even with immediate repair, a study has shown that 45% of repaired exposed tubes required a second operation, and 13% eventually needed the tube removed.3 In certain situations, if the tube is only partially exposed or a small conjunctival defect exists over the plate, medical management can be considered, which includes antibiotic ointment prescribed two times per day, a topical antibiotic three to six times a day and a trial of doxycycline tablets 50mg to 100mg twice per day (to assist in healing). If the examination results are the same after one to two weeks of medical management, a referral for repair or removal will be needed.
As the primary provider of glaucoma care for many patients, optometrists play a critical role in the postoperative management of these surgeries. “Advanced glaucoma patients with glaucoma drainage devices are in many of our clinics, and these devices can have early or late complications, including tube erosions,” Dr. Schweitzer says. “Many of these patients will do well if the erosion is recognized early and repaired.”
Dr. Ajamian is board certified by the American Board of Optometry and serves as Center Director of Omni Eye Services of Atlanta. He is vice president of the Georgia State Board of Optometry and general CE chairman of SECO International. He has no financial interests to disclose.
1. Gedde SJ, Schiffman JC, Feuer WJ, Herndon LW, Brandt JD, Budenz DL. Treatment outcomes in the Tube vs. Trabeculectomy (TVT) study after five years of follow-up. Am J 2. Ophthalmol. 2012;153;(5):789-803. 2. Wishart PK, Choudhary A, Wong D. Ahmed glaucoma valves in refractory glaucoma: a seven-year audit. Br J Ophthalmol. 2010;94(9): 1174-9. 3. Huddleston SM, Feldman RM, Budenz DL, et al. Aqueous shunt exposure: a retrospective review of repair outcome. J Glaucoma. 2013;22(6):433-8. |